

What's Longevity Medicine? • Nobel Prize for Immune System • Human Metabolism Map • Digital Twin
Issue 66: The front page of longevity medicine - curated by doctors, for doctors.

Hey Doc,
This morning I finally opened three saved reads: the Nobel Prize in Medicine, a study on the largest genetic map of human metabolism, and Eric Topol’s latest. The takeaway was clear: longevity medicine isn’t fringe anymore. But what does “longevity medicine” actually mean? So I dug in and wrote a longer piece, inspired by King Gilgamesh, Goddess Elbe, and the Taoist quest for immortality, to explore where this dream of living longer truly began, and how it has evolved into what we now call longevity medicine.
At the end of the day, we all want to live a good life!
Healthy sunday!
Dr. David Luu
Founder, Longevity Docs
www.longevitydocs.org
In this week newsletter:
Cover Story: What’s Longevity Medicine?
Buzz in the Chat: GLP1s & SIBO • WHOOP’s Labs & AI • Testosterone range
Research Radar: Human Metabolism Map • Transformer-based models
Longevity in the News: Nobel Prize • Digital Twin
Longevity Intelligence: SoulCycle + Superpower • Wisp + Vesalius

Each week, I try to explore one idea that could advance longevity medicine and hopefully support physicians in bringing it to life.
What Is Longevity Medicine - From Origins to Futurism
The desire to live longer and better is as old as humanity itself. From the Epic of Gilgamesh to the Taoist search for immortality and the Greek idea of bios kalos, meaning “the good life,” every civilization has sought to stretch time. Longevity is not marketing; it is the aspiration of every civilization and empire.
Science (antibiotics, vaccines, surgery, sanitation, public health) made us live longer. Yet the modern plagues (heart disease, cancer, neurodegenerative disease) won’t yield to lifestyle tweaks alone. They demand new advanced holistic approaches and therapies.
If we are serious about longevity on a global scale, we must combine prevention, technology, and biology to overcome the limits of behavior and access.
In the 20th century, Élie Metchnikoff, a Nobel laureate at the Pasteur Institute, transformed this ancient dream into science. He proposed that aging is not destiny but a biological process that can be studied, slowed, and perhaps reversed. His belief that “aging begins in the gut” anticipated today’s microbiome research and our systemic view of health.
Today, that dream has evolved into longevity medicine, a discipline born at the intersection of biology, technology, and human aspiration.
If traditional medicine was built to manage disease, longevity medicine exists to manage health and unlock potential.
The former asks, “What’s wrong?” The latter asks, “What’s possible?”
What Longevity Medicine is and is not
Associating longevity medicine to supplements, IV drips, or stem cells is a misunderstanding, or worse, a cheap caricature. It is like reducing cardiology to managing cholesterol with statins.
Modern cardiology now measures ApoB, Lp(a), and sterols to understand lipid absorption and degradation. It visualizes plaque morphology with AI-powered CT angiogram and tracks VO₂ max and visceral fat with DEXA. It uses ezetimibe, PCSK9 inhibitors, GLP-1 receptor agonists, and EPA to personalize therapy.
This is not alternative medicine; it is evolution, where precision, personalization, and prevention work together, guided by data, evidence, and empathy. Longevity medicine applies that same rigor to every system of the body, not to chase immortality but to preserve function and extend vitality.
The era of predictive longevity
For a century, medicine has been reactive, diagnosing too late, intervening too late, and defining success by survival rather than vitality. Prevention has often meant early detection, not true interception. A new era is emerging, one defined by precision monitoring, continuous data, and predictive intelligence.
As Eric Topol described in Ground Truths, primary prevention, the ability to avert disease before it begins, has long been an unmet promise. Until now. The convergence of AI, biomarker science, and continuous biosensing is finally making it achievable.
Large health models will forecast the likelihood and timing of more than one thousand diseases by learning the grammar of biology. Combined with continuous protein monitoring, organ aging clocks, polygenic scores, and AI-powered personal health agents, medicine is evolving from snapshots to a living, adaptive ecosystem.
This is the blueprint for predictive longevity medicine, where health becomes a dynamic dashboard and every data point tells the story of how the body is aging and adapting.
In this world, the physician becomes a navigator of biological potential, fluent in both algorithms and empathy, data and ethics. Patients will not come seeking miracles but meaningful interpretation. Longevity medicine is not a product; it is a new operating system for health that is continuous, predictive, and profoundly human.
Medical truths evolve
As Sir William Osler said, medicine is “a science of uncertainty and an art of probability.” Unlike physics, medicine deals with living systems that respond differently depending on genetics, environment, emotion, and time. What we call truth in medicine is rarely absolute; it is a consensus built on the best available evidence, always open to revision.
Empirical truth: measurable fact.
Clinical truth: consistent human outcomes.
Consensus truth: accepted understanding.
Personal truth: what works for the individual.
Longevity medicine lives at the frontier between consensus and emerging empirical truth, embracing uncertainty as the engine of discovery.
What must be improved: the honest reckoning
Longevity medicine holds immense promise and real risk. The field must confront both.
Access and equity. Today, longevity medicine is a luxury good. Advanced testing, latest therapies, and specialized physicians are available mainly to the wealthy, while those with the greatest need, communities with shorter life expectancy, remain excluded. The original promise of medicine was democratization through antibiotics, vaccines, and public health. Longevity medicine must not reverse that legacy. True longevity cannot exist in a world where some live to ninety with vitality while others die at sixty from preventable disease.
Overmedicalization. The more we measure, the more we find, and the more we feel compelled to treat. Innovation brings value but also risk, turning the healthy into the perpetually managed. A genetic risk is not a disease, and a drifting biomarker is not pathology. The field must learn restraint, knowing when to act, when to observe, and when to accept uncertainty. Many interventions recommended today will not stand the test of time.
Distinguishing evidence from aspiration. The frontier is thrilling, but excitement is not evidence. Cardiovascular optimization, metabolic health, cognitive engagement, and community-based longevity are proven. AI prediction, continuous protein monitoring, and senolytics are promising but unproven. Cellular reprogramming remains experimental. Longevity medicine earns credibility by distinguishing what is possible from what is proven and by refusing to commercialize hope.
The future of longevity medicine belongs to those who can dream without deceiving, inspire without overselling, and recognize that the limiting factor is rarely knowledge but the implementation of what we already know works.
The role of the longevity doctor
True longevity doctors are not defined by title but by literacy in the science of human performance and aging. They balance promise and limitation, benefit and risk, evidence and empathy. They do not sell hope; they translate science into wisdom. They do not deny curiosity; they guide it responsibly. They do not treat disease; they cultivate potential.
I don’t believe longevity medicine should be a specialty. It is a philosophy of care that merges ancient wisdom, modern diagnostics, and human compassion, an evolution of evidence-based medicine toward function over pathology, resilience over repair, and health/life optimization.
Every doctor should be a longevity doctor. Within a few years, longevity medicine won’t be a niche, it will be primary care by default.
The soft power of a definition
No agency, company, or guild owns “longevity medicine.” Its meaning is emerging in culture and practice. Pioneers are experimenting; skeptics are observing; the field keeps moving.
Some call it anti-aging, concierge, functional, integrative, regenerative, or precision medicine. But as the Greeks once said, it is simply good medicine, bios kalos.

Every week, the Longevity Docs WhatsApp group feels like a front-row seat to the future of medicine. Here’s what had doctors buzzing:
Wearables x Labs: WHOOP’s AI Coaching Goes Clinical
Longevity Docs discussed WHOOP’s new lab integration and AI-generated guidance (sleep debt, alcohol intake, T/SHBG cutoffs), plus demand for faster access from the waitlist. Pricing for the 65-biomarker panel raised eyebrows versus Quest contracts/Medicare copays.
Key Takeaways for Doctors:
Wearables are moving from “tracking” to interpreting labs + behavior in-app.
Expect patient questions on “optimal vs sufficient” testosterone bands (incl. free T, SHBG).
Access is rolling out in batches; clinicians want admin channels for patient onboarding.
GLP-1 Protocols: SIBO or Not?
Lively debate: some report GLP-1s “set up” GERD/SIBO; others argue the mechanism is conflated (gastric emptying ≠ MMC impairment) and note microbiome benefits and anti-inflammatory effects. Several shared playbooks (protein targets, resistance training, DEXA, micronutrient and hormone checks) and adjuncts (CJC/Ipamorelin/Tesamorelin, amlexanox, LDN, tesofensine).
Key Takeaways for Doctors:
Separate early-phase GI symptoms from true SIBO; consider breath testing when indicated.
Create structured GLP-1 follow-up: protein, training, DEXA, sleep, micronutrients, hormones.
Risk/benefit is clearer in disease populations than “biohacker” optimization.
Testosterone: Grade It, Don’t “In-Range” It
A popular framing: quartile-based “report cards” (A-F) for total/free T tied to CV outcomes to improve patient understanding and motivation. Strong emphasis on lifestyle first (sleep, adiposity, OSA, training, alcohol) before TRT, especially in younger men (fertility risks).
Key Takeaways for Doctors:
Use free T and SHBG with total T; explain trade-offs of TRT (HPG suppression, sperm).
Lifestyle changes can lift T and global risk simultaneously; try before TRT when appropriate.
Join 500+ Longevity Docs Across 50 Countries
Longevity Docs is a highly vetted, invitation-only community for physicians shaping the future of longevity medicine. Apply online and connect 1:1 with our team

Each week, I highlight a few studies that caught our eyes and could shape the future of longevity medicine.
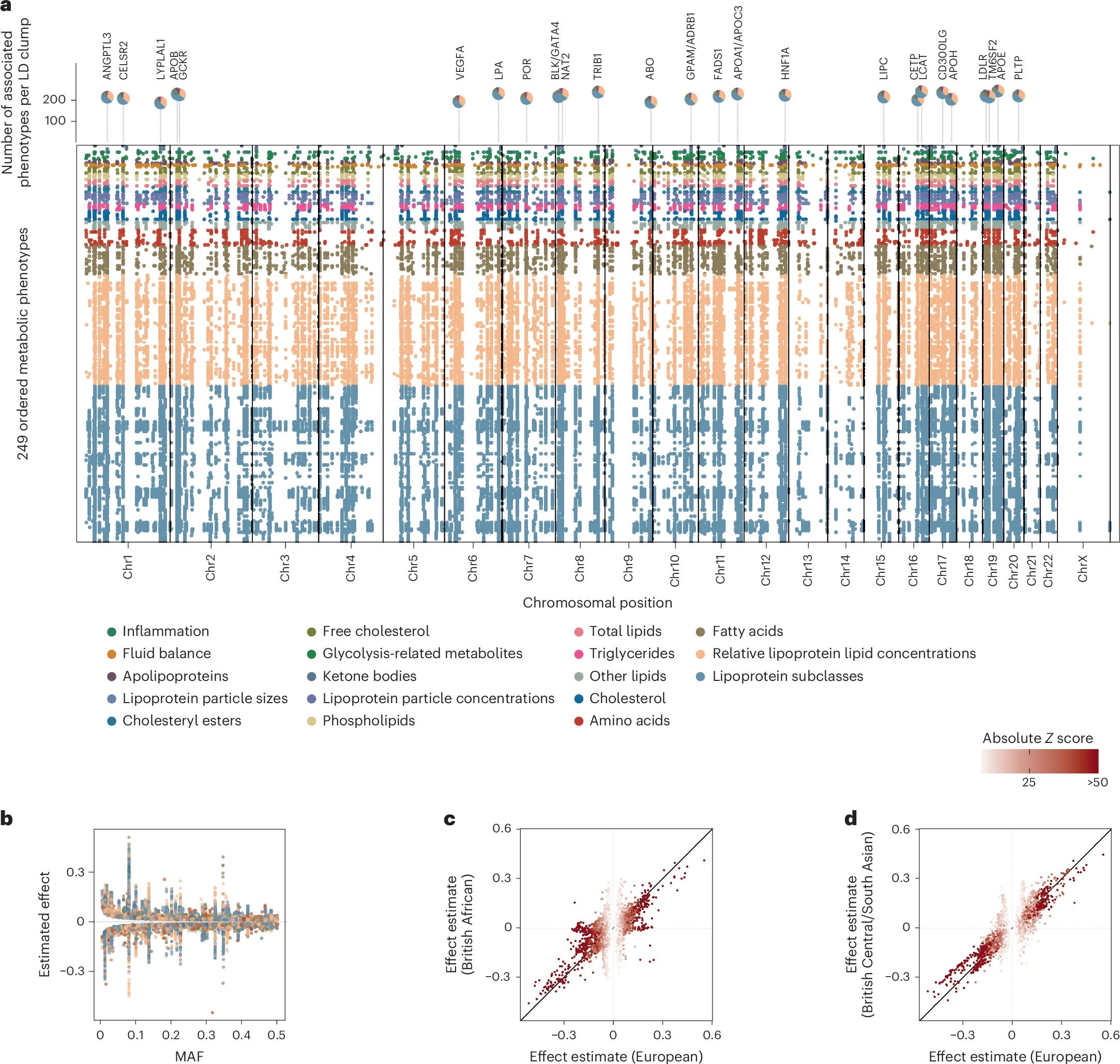
A genetic map of human metabolism across the allele frequency spectrum
Now, the largest genetic map of human metabolism has been created, revealing new insights on the role of metabolites in health and disease and creating a blueprint for further research. Nature Genetics
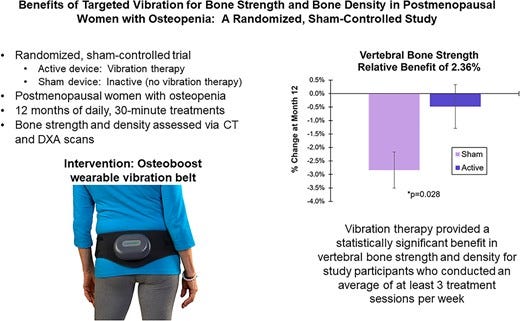
Benefits of Targeted Vibration for Bone Strength and Bone Density in Postmenopausal Women with Osteopenia: A Randomized, Sham-Controlled Trial
The vibration therapy was well-tolerated, and there were no serious device-related adverse events. These results demonstrate that targeted vibration is safe and, in adherent individuals, can significantly mitigate the decline in vertebral bone strength and vertebral bone density in postmenopausal women with osteopenia. JBMR
Endogenous Testosterone and Mortality Due to All Causes, Cardiovascular Disease, and Cancer in Men
In men, endogenous testosterone concentrations are inversely related to mortality due to cardiovascular disease and all causes. Low testosterone may be a predictive marker for those at high risk of cardiovascular disease. Circulation
Learning the natural history of human disease with generative transformers
Transformer-based models appear to be well suited for predictive and generative health-related tasks, are applicable to population-scale datasets and provide insights into temporal dependencies between disease events, potentially improving the understanding of personalized health risks and informing precision medicine approaches. Nature

I comb through the mainstream headlines, handpick the most relevant longevity stories.
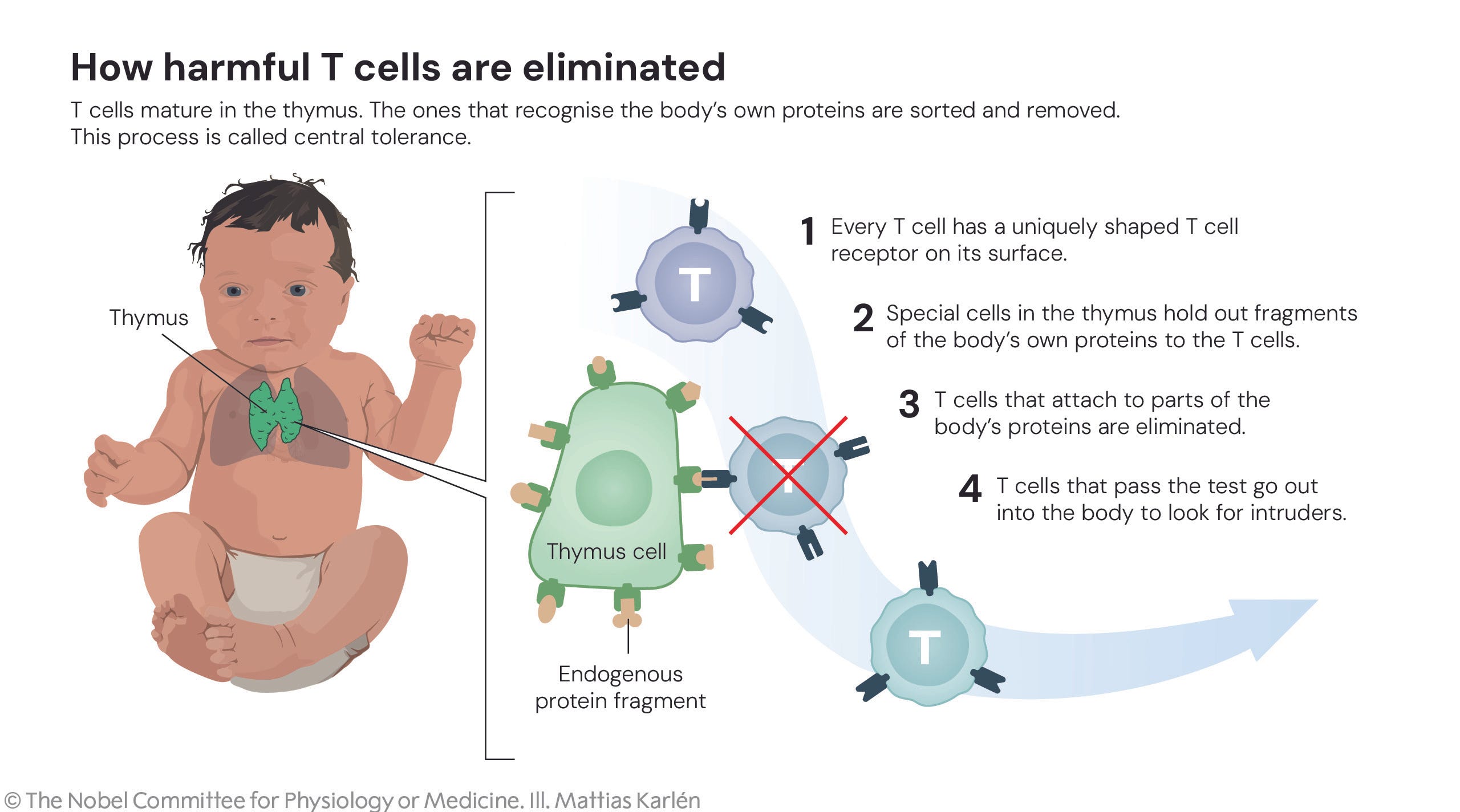
Nobel Prize in medicine goes to trio of scientists for discovering how the immune system is kept in check
Researchers long believed they knew the answer to these questions: that immune cells mature through a process called central immune tolerance (see image). However, our immune system turned out to be more complex than they believed. Mary Brunkow, Fred Ramsdell and Shimon Sakaguchi have been awarded the 2025 Nobel Prize in Physiology or Medicine for their discoveries concerning peripheral immune tolerance. CNN
AI and the Fountain of Youth
AI + biology are moving longevity from sci-fi to clinic, with a realistic shot at adding a decade of healthy life. Early signals (e.g., engineered stem cells/exosomes in primates) plus AI-accelerated drug design point to prevention before symptoms.
Continuous monitoring and “hospital-at-home” will prioritize healthspan over lifespan.
But skip the hype: insist on rigorous trials and update policy (retirement, insurance, equity) for a longer-living society. WSJ
Digital Twin: How Tracking Your Health Metrics Can Help You Live Longer
Dr. Zahi Fayad of Mount Sinai envisions a future where continuous health tracking reshapes medicine. His Digital Twin Study uses wearables, sensors, and imaging to build real-time models of human health, predicting disease before symptoms appear. Participants are monitored through Oura Rings, glucose sensors, spirometers, and quarterly blood tests to map physiological and molecular data. Time

Social Ties Help You Live Longer. What Does That Mean for Introverts?
You don’t need to be extroverted to live longer, just connected. Research shows longevity gains come from quality, not quantity, of relationships. Emotional and logistical support, healthy habits, and mental stimulation from social interactions all protect against inflammation and disease. For introverts, even small, meaningful exchanges -a walk with a friend or a chat at a café- can nurture longevity as powerfully as big social circles. NYT

Every week, I track the biggest moves in longevity: new funding rounds, partnerships, product launches, and key hires.
SoulCycle Teams With Superpower To Integrate Biomarker Testing
Fitness and healthcare continue to merge as telehealth platform Superpower joins SoulCycle’s Fall Challenge to bring biomarker insights into the cycling studio. Athletech News

Wisp, Vesalius partner to bring peptides into women’s healthcare space
Women’s telehealth company Wisp announced a strategic partnership with Vesalius Longevity Labs, a company that provides regenerative medicine, to develop an exclusive range of peptide therapies aimed at advancing women’s quality of life and promoting longevity. Mobihealthnews

Monarch Athletic Club Enters Miami
Monarch’s gym-meets-clinic integrates preventative care with prescriptive fitness, offering healthspan optimization spanning peptide treatments, contrast therapy, PT, and strength training. Fitt Insider

Longevity Docs AI/Tech Mastermind
New York City & Virtual | January 17, 2026
Longevity Docs Summit Cannes
Cannes, France | June 10-11, 2026
Longevity Docs Around the World
Meet us at the following events:
Riyadh · October 24–26 — Zenos Health Summit
New York · October 30 — Galien Patient Summit
Miami · November 12 — Longevity Docs Table
Novato · December 6-8 — Longevity Clinic Roundtable
Vegas · January 6-9 — CES
Conferences Calendar
Health Optimization Medicine Symposium: Boulder, October 17-18
Biomarkers of Aging: Boston, October 20-21, 2025
Eudemonia: Palm Beach, November 13-16
A4M: Las Vegas, December 12-13

Why every doctor should be a longevity doctor.
The Movement
Longevity Docs is the world’s leading collective of physicians advancing longevity medicine through education, clinical research, advisory, and exclusive experiences. With over 400 members in 50+ countries, we’re building the global infrastructure for evidence-based, personalized longevity care.

Why “Longevity Docs”?
Because we believe longevity is not a specialty — it’s a human right.
The future of medicine is proactive, not reactive. It's interdisciplinary, not isolated. It’s collaborative, data-driven, and deeply human. And it starts with us — the physicians who dare to redefine what care looks like across the decades of a patient’s life.
“Longevity Docs” isn’t just a name. It’s a statement of purpose.
Our Ecosystem
Physician Network
A trusted global collective of longevity-focused doctors exchanging protocols, referrals, and real-world clinical outcomes.Education & Certification
Earn your Certified Longevity Doctor™ designation through our advanced curriculum, live masterclasses, and continuous learning tracks.Decentralized Research
Lead or participate in multicenter clinical trials and patient registries, accelerating evidence generation for healthspan optimization.Strategic Advisory
We partner with vetted longevity companies, life-science, tech, and clinics to help them grow.Global Events & Experiences
Access exclusive gatherings like the NYC Mastermind and the Cannes Longevity Summit & Awards
Who It’s For
Doctors → Join the club, get certified, grow your practice
Health Systems → Implement clinical longevity programs
Brands & Startups → Validate products, find advisors, run trials
Investors → Gain early access to insights, doctors, and deal flow
We’re not just witnessing the transformation of longevity medicine we’re building it. Together.
Subscribe to the Longevity Docs Newsletter
Stay connected with the backstage of the Longevity Docs community, a network of over 500 physicians spanning 50 countries, united in our mission to democratize longevity medicine. Explore the latest in evidence-based longevity care, gain exclusive access to physician insights, and join us in shaping the future of this transformative field.
Newsletter Disclaimer:
I’m not too kean on overemphasis on vitamins and medication for longevity sake. Let’s focus on social aspects of life of centrarians