

Welcome to Hippo: AI learning Assistant for longevity medicine
#81 Weekly Longevity Medicine Intelligence

Hey Doc,
Welcome to the home of longevity medicine!
What I saw: Last week we gathered 100+ physicians in NYC for our AI & Tech Mastermind. The question on the table: how will doctors use AI or will they be replaced? Full room Network + knowledge + ambition in one room. Felt super inspired, thank you to our amazing faculty from Mount Sinai, Mayo Clinic, Buck Institute, Stanford, NYU, and all the longevitydocs!
What I heard: Longevity medicine is showing up in every conversation now. Large companies. Regulators. Tech. Media. I met with several of them this past few weeks. They are all looking for the same thing: ethical, trained longevity doctors who can deliver safe, evidence-based, personalized care at scale. They are looking for us.
What I think: Medicine is having a reckoning. The future generation of physicians will carry a mission: leveraging technology and education to keep humanity healthy for longer. To add a layer of longevity care on top of healthcare. And I am so optimistic about this.
Every doctor will eventually be a longevity doctor.
And every doctor should be a good human first.
Happy sunday!
Dr. David Luu - Founder, longevitydocs.™
PS: few pics from our Mastermind










Each week, I try to explore one idea that could advance longevity medicine and hopefully support physicians in bringing it to life.
Hippo: the AI learning assistant for certified longevitydocs (Beta Launch)
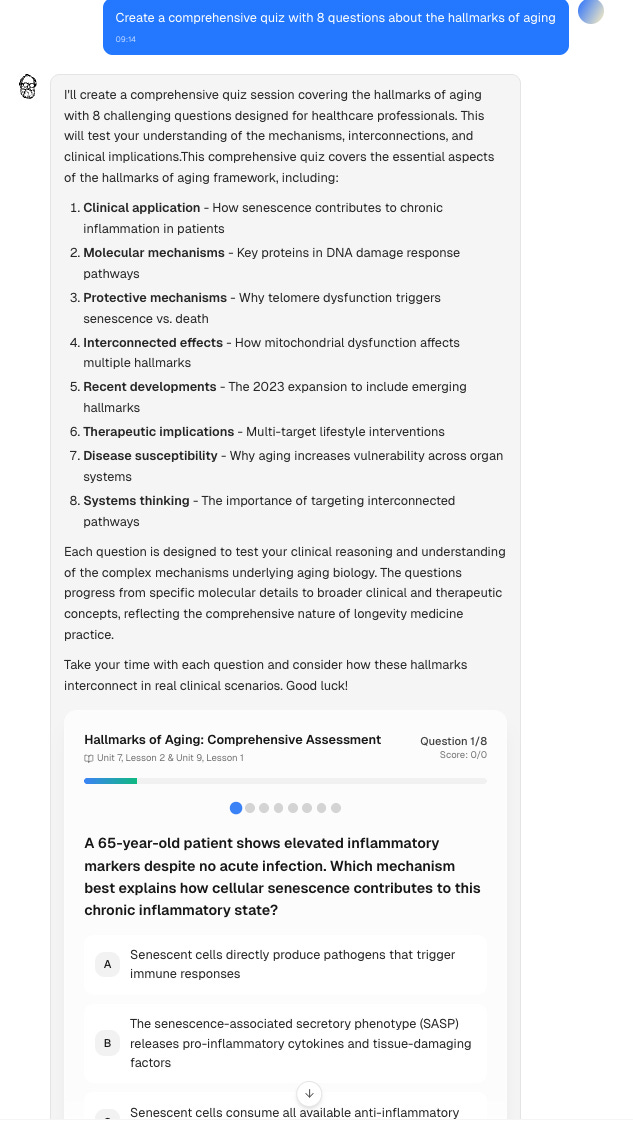
This morning I opened Hippo and asked it to create a Quiz session. Within minutes I'd tested my knowledge, found a gap I didn't know I had, and moved on with my newsletter. A quick, focused way to build longevity fluency.
Why Hippo?
What if every physician had access to rigorous longevity education, on demand, wherever they are?
This is what democratizing longevity medicine looks like. Not discounting it. Making it accessible, rigorous, and built into daily knowledge rituals that compound over time.
Hippo is an AI learning assistant built on the Certified Longevitydocs curriculum. Ask anything about the CLD course. It meets you where you are: quizzes, clinical questions, flashcards, deep explanations, summaries. All grounded in our knowledge base.
Learning medicine differently
Books, conferences, videos, all valuable. But I want to learn differently: convenient, playful, engaging, challenging, and always on.
Longevity-specific knowledge: You were trained in pathology. Hippo teaches through aging mechanisms, healthspan and prevention: the way longevity medicine actually works.
Fill the gaps: Your patients are asking about GLP-1s, rapamycin, Lp(a). Hippo closes the gap between what they’re reading and what you can confidently answer … in five minutes, from our curriculum.
Shorten the implementation time. Reading a concept is one thing. Applying it Monday morning is another. Hippo equips you with the confidence you need.
What we are testing in our beta
We imagine an assistant that helps you learn faster and deeper. Our beta version is testing:
Quiz Sessions: clinical reasoning questions
Open Questions: write detailed answers to realistic case scenarios. Hippo evaluates your reasoning and highlights where to strengthen.
Flashcards on biomarkers, mechanisms, interventions. Organized by difficulty and clinical relevance.
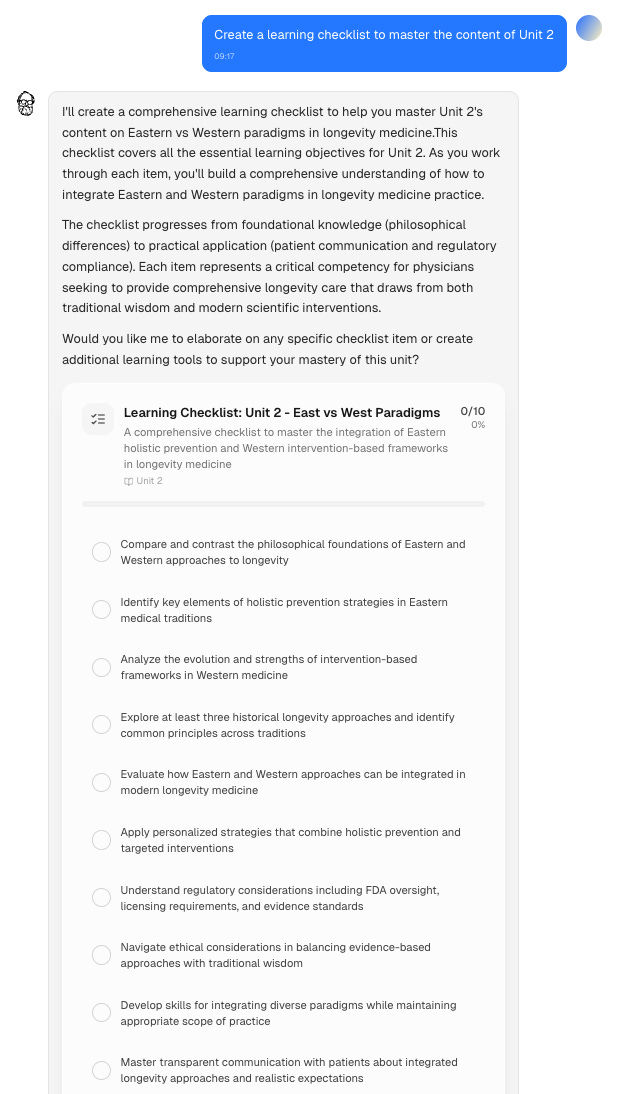
Learning Checklists to track your knowledge unit by unit. See what you’ve covered. See what’s left.
Explain: ask Hippo to break down any concept. Structured, curriculum-sourced, deep.
Summary: get a key takeaways on any topic. Fast.
This is a beta. We’re building it alongside our physician learners. Your feedback shapes what Hippo becomes. And what longevity medical education could look like in the future.
CLD from New York. Geneva. Dubai. Accra. Singapore. Wherever you’re learning, Hippo’s there.
Every doctor should be a longevity doctor.
Now, every certified longevitydocs has Hippo.

Every week, the Longevity Docs WhatsApp group feels like a front-row seat to the future of medicine. Here’s what had doctors buzzing:
Skin longevity protocols anyone?
Two dermatologists, a regenerative medicine specialist, and a dozen longevity docs shared their actual routines. The conversation moved through three evidence tiers: foundational, advanced, and devices.
Foundational tier (universal): retinoids, vitamin C, and mineral-based SPF showed up in every single protocol. No debate here.
Advanced (growing adoption): compounded formulas combining rapamycin, estriol, and GHK-Cu copper peptide are increasingly common. Exosomes came up repeatedly. Re-Q (mTORC1 inhibitor) is underrated.
Devices (most debated): Ultherapy vs. Sofwave vs. Fraxel showed real practitioner disagreement. Pain/downtime vs. results vs. maintenance frequency.
Biggest mistake: layering too many actives and destroying skin barrier. Less is more.
“The mTOR inhibition data for skin aging is solid, and I’m seeing visible improvement in fine lines and texture after 6 months.”
“Less is more. Pick 3-4 evidence-based interventions and stay consistent.”
Rapamycin for ovarian reserve?
Emerging protocols using rapamycin + PRP for diminished ovarian reserve sparked intense discussion.
Can mTOR inhibition restore reproductive aging in real time?
Key takeaways
one doc protocol: 5mg rapamycin weekly + ovarian PRP, with 6/8 patients showing AMH improvement over 6 months (SR’s protocol)
LDN synergy: 4.5mg LDN nightly + 3mg rapamycin weekly in women with PCOS and early ovarian aging (SZ’s protocol)
Mechanistic rationale: mTOR inhibition may restore autophagy in aging oocytes and improve mitochondrial function in follicles
Still experimental: position as adjunctive to standard fertility treatments, not standalone. Track AMH, FSH, AFC, symptom logs.
Caution: rapamycin’s immunosuppressive effects are a concern in women trying to conceive. Track infection risk.
I’m tracking everything:AMH, FSH, AFC, symptom logs. We may be writing the playbook in real time.
Genetic testing for longevity
SM’s recommendation of whole genome sequencing via New Amsterdam Genomics sparked debate on what’s clinically useful versus what’s noise. The consensus on minimum testing crystallized, but the data security question hit a nerve.
Are we ordering genomic data we can’t interpret yet—and then losing access when companies shut down?
Key takeaways
Minimum: APOE genotyping (every longevity patient), cancer predisposition panels (BRCA, Lynch, TP53 if family history), pharmacogenomics (CYP450 variants)
WGS debate: only for unexplained symptoms/rare disease vs. data banking for future interpretation. Most findings are VUS (variants of uncertain significance).
Clinical utility limited today: in 5 years, today’s VUS may be tomorrow’s treatable risk, but we’re not there yet
Data security unresolved: patients’ genomic data becomes inaccessible when companies shut down or get acquired
Action: tell patients to download raw data files immediately and store them independently. Data portability is the patient’s responsibility.
“The question everyone’s avoiding: what happens to your patient’s genomic data if the company folds? We don’t have a good answer yet.”
Not a member yet? Join longevitydocs™
We're a physician-only network. Curated. Vetted. Built on trust. If you're committed to practicing longevity medicine with rigor, peer support, and shared standards → this is your community. Apply to connect with our team.

A Placebo-Controlled Trial of the Oral PCSK9 Inhibitor Enlicitide
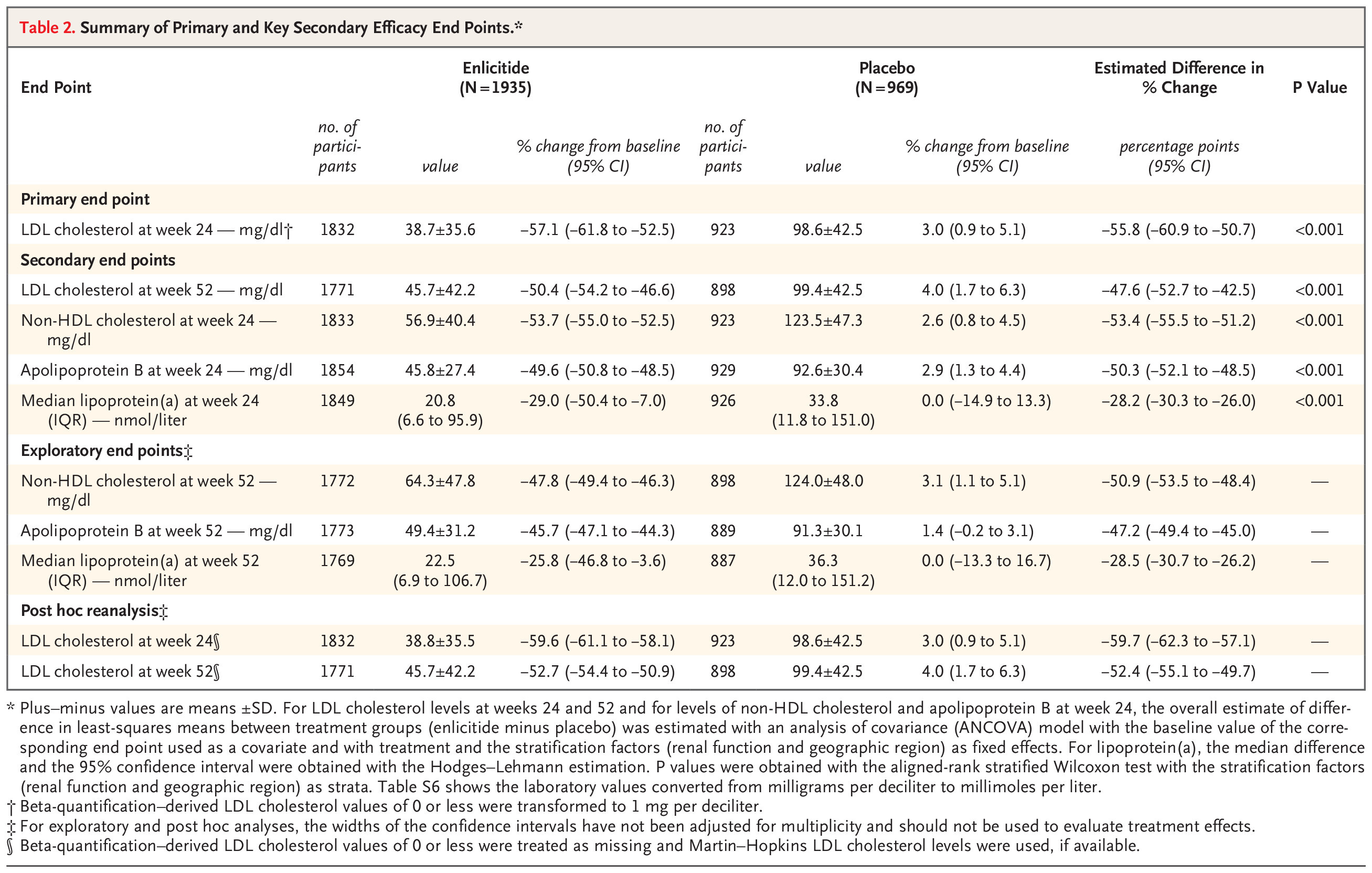
Enlicitide is the first oral PCSK9 inhibitor — a once-daily pill. In the CORALreef Lipids trial (2,909 patients, 52 weeks), it delivered a 57% reduction in LDL cholesterol, on par with injectable options like evolocumab and alirocumab. It also significantly lowered apoB, non-HDL cholesterol, and — notably — lipoprotein(a) by 28%, a genetically determined risk factor that until recently had no effective pharmacological intervention. Safety was clean. Adherence was 97%. NEMJ
The Inherited Basis of Coronary Artery Disease
Comprehensive NEJM review synthesizing decades of genetic research on CAD. Twin studies show 50% heritability. Since 2007, large-scale genotyping identified hundreds of genetic variants. Polygenic risk scores now show 3-5x higher risk for those in top 5% vs average. Key insight: some associated genes already constitute treatment targets; others point to unexplored disease mechanisms.
Polygenic risk scores for CAD should be part of longevity assessment for patients with family history of early cardiovascular disease—especially valuable for those with “normal” lipids/BP who may still carry high genetic risk.
Statin Safety: Product Labels vs. Clinical Trial Evidence
Meta-analysis of individual participant data from large double-blind RCTs challenges adverse effect claims listed in statin product labels (based mainly on non-randomised, non-blinded studies subject to bias). Study examined undesirable effect terms listed in SmPCs for five statins (atorvastatin, fluvastatin, pravastatin, rosuvastatin) by analyzing actual double-blind trial data.
Statin product labels may overstate adverse effects based on weak observational data - double-blind RCT evidence shows better safety profile than labels suggest. Use this when counseling patients hesitant about statin therapy due to label warnings. The Lancet

Every week, I track funding, FDA approvals, product launches, and breakthrough announcements shaping longevity medicine.
AI/TECH
Lotus Health Launches Free Primary Care with AI Doctors

Lotus Health secured $35M Series A to build 24/7 AI-enabled primary care that’s completely free to patients. Board-certified physicians from Stanford, Harvard, and UCSF oversee AI-generated diagnoses. Business model: “premium sponsorships” in-app rather than billing patients or insurance. Claims 10x more patients than traditional practices.
CARE
Radiology practice SimonMed Imaging launches new ‘longevity screening’ division

SimonMed Imaging rebranded and launched SimonMed Longevity, a new division offering whole-body MRI and multi-modality preventive screening powered by 3T MRI technology and AI-enabled imaging. The service launched at 30 locations nationwide, expanding to 70+ sites by Q1 2026, and integrates the company's previous simonONE whole-body MRI program into its main brand.
POLICIES
Hims to stop offering GLP-1 pill after FDA warned of crackdown

FDA announced it will restrict GLP-1 ingredients in compounded drugs after Hims launched $49 compounded semaglutide pill. Novo Nordisk is suing. HHS referred Hims to DOJ for investigation. Key: semaglutide is off the FDA shortage list, removing the legal basis for compounding.
BIOTECH
Life Biosciences Gets FDA Clearance for Age-Reversal Trial

Life Biosciences, cofounded by Harvard’s David Sinclair, received FDA approval for Phase 1 trial of partial epigenetic reprogramming to restore vision in glaucoma and NAION patients. Uses three Yamanaka factors to rejuvenate cells without full pluripotency reset. First patients enrolling in next few months.

Conferences
Feb 19–21 — IH Symposium · New York, NY Integrative health leaders meets
Feb 27–28 — CALM · Fort Lauderdale, FL Clinical approaches to longevity medicine.
Jun 9–11 — Longevity Docs Summit · Cannes, France Our flagship. Physicians, researchers, innovators, investors, policymakers — one stage.
Jun 29–Jul 1 — A4LI H-SPAN Summit · Washington, DC Longevity medicine meets regulation and policy.
Aug 24–28 — ARDD · Copenhagen, Denmark Where aging research meets drug discovery.
Oct 17 — Longevity Docs Skin Longevity Mastermind · New York, NY. Curated physicians. Deep science. One room.
TBA — Longevity Clinics Roundtables · Buck Institute Clinical practice meets research infrastructure.
Books
I wanted to share 3 upcoming books from Amy Shah, MD, Florence Comite, MD, and Michael Clinton. Excited for the community to keep educating and raising awareness


The Professional Infrastructure for Longevity Medicine
longevitydocs.™ is the professional infrastructure for longevity medicine: a physician-only network uniting 600+ physicians across 50+ countries. We build the network, education, research, and culture that make longevity medicine the new gold standard of care.
Longevity medicine is the personalized, evidence-based practice of modifying the root mechanisms of aging (biological, cognitive, and psychosocial) before they become disease, extending healthspan, not just lifespan. Using advanced diagnostics, precision interventions, and AI-enabled monitoring, it translates measurement into action across every medical discipline. Success is measured in functional capacity, vitality, and disease-free years.

Our Pioneering Approach: Network, Education, Research, Culture
Professional Network: A curated, physician-only circle of trust. Leading longevity physicians share protocols, collaborate on clinical challenges, and elevate each other across borders, specialties, and cultures. Shared intelligence as infrastructure.
Medical Education: The Certified longevitydocs™ (CLD) is the first structured, physician-led clinical curriculum for longevity medicine. Comprehensive, evidence-based, and practice-ready. Continuous education programs delivered through structured cohorts and institutional partnerships worldwide.
Clinical Research: A clinical research infrastructure enabling rapid generation of real-world evidence across the longevitydocs™ network. Patient registries, standardized outcome measurement, and multi-center collaboration frameworks that transform everyday practice into coordinated discovery.
Cultural Experiences: From Cannes to New York, our Summits, Awards, Masterminds, and Jefferson Dinners convene top researchers, clinicians, investors, and government officials to shape longevity medicine’s growth, investment, and policy. We write the story of longevity medicine for the world.
Intelligence: Weekly syntheses of scientific breakthroughs, clinical best practices, business signals, and global market analysis; the industry’s trusted source of strategic intelligence for physicians, institutions, and Fortune 500 companies.
Subscribe to the Longevity Docs Newsletter
Longevity medicine is moving fast. Every week, we bring you what matters: clinical insights, research signals, and perspectives from 600+ physicians across 50+ countries. One newsletter. Built for the physicians shaping this field.
Newsletter Disclaimer:
Thank you, this is a smart “welcome” post! It frames Hippo as an assistant for learning and synthesis, not as a replacement for judgment. The real value of an AI learning assistant isn’t that it can answer, but it’s that it can reduce friction on the parts of learning that waste time without adding understanding: finding primary sources, translating dense mechanisms into mental models, and helping people test their own reasoning (“What would change your mind? What’s the counter-evidence? What’s the base rate?”).
A few things I especially appreciate (and hope you continue to emphasize as Hippo evolves):
1. Evidence hygiene built into the workflow: citations to primary literature, clear labeling of uncertainty, and a “show me the source” default.
2. Guardrails against overconfidence: flagging when an answer is extrapolation vs human outcome data, and prompting for clinician review when users drift into individual medical decisions.
3. Privacy + clinical realism: strong messaging that personal health details shouldn’t be treated casually, and that “helpful” doesn’t mean “diagnosing.”
If Hippo consistently nudges users toward better questions, not just faster answers, but it’ll be genuinely additive to medical education and patient literacy. Excited to see where you take it!