

The Longevity Tourism Boom
#98 Weekly Longevity Medicine Intelligence


Hey Doc,
Thank you for your patience. I took some time off after Cannes to recharge with my family, catch up with friends, eat Mediterranean food, discover new places and enjoy life. I am writing this week newsletter just coming back from Florence, the capital of the Renaissance. A city built by the Medici, who were essentially the original venture capitalists, backing artists, architects, and scientists the way we fund startups today. And one of those bets was Leonardo da Vinci.
Dav dissected the body of an elderly man in Florence to understand why his vessels had changed. He described thickened arterial walls, narrowed lumens, and reduced blood flow. He drew it. He documented it. Four hundred years before we had the word atherosclerosis. A painter, sitting in a morgue, doing vascular biology because he was curious.
This newsletter is my reflection on what is happening with longevity hospitality globally, and specifically the longevity tourism boom that is reshaping how people access (or think they are accessing) medicine around the world.
Dr. David Luu, Founder, longevitydocs.™
PS: few memories and longevity tourism

Each week, I try to explore one idea that could advance longevity medicine and hopefully support physicians in bringing it to life.
The Longevity Tourism Boom
Longevity spa, longevity retreats, or longevity checkup. Longevity is everywhere. A hotel in the Swiss Alps is selling a “longevity suite” with cryotherapy and IV drips. A resort in Bali is packaging breathwork and cold plunges as longevity medicine. A clinic in Bangkok is offering full-body MRI screenings to tourists between temple visits. A facility in the Cayman Islands is offering stem cells at $25,000 per session.
The word longevity is now a travel category.
This is not new.
People have always traveled for health. Romans soaked in the hot springs at Bath. European physicians in the 1800s prescribed entire seasons at Baden-Baden, Vichy, and Karlovy Vary. Baños de Agua Santa in Ecuador built an economy around volcanic thermal springs centuries before anyone used the word longevity. The Swiss sanatoriums treated tuberculosis with mountain air and structured rest. The Dead Sea has been a medical destination for skin disease for over two thousand years.
The instinct to travel toward health is ancient. What is new is the scale, the marketing, and the clinical distance between what is being sold and what is being supervised.
The four levels of longevity tourism
Not all longevity tourism is the same. The category now spans four distinct tiers, each carrying a different risk profile.
Level 1: Hotel and spa programs. This is the entry point. A luxury hotel adds a “longevity menu” to its spa: cryotherapy, infrared saunas, IV vitamin drips, red light therapy, metabolic smoothies. The interventions are mostly low-risk. The medical supervision is mostly nonexistent.
Level 2: Retreats. A step up in duration and intention. Five to fourteen days. Structured programs with breathwork, meditation, cold exposure, movement, nutrition, and sometimes basic lab work. The best ones have medical directors and structured intake. The worst ones package the same activities under a longevity label with no clinical oversight and no follow-up after checkout.
Level 3: Diagnostic tourism. This is growing fast. Patients flying to South Korea, Thailand, or Dubai for comprehensive health screenings: full-body MRI, coronary calcium scoring, cancer biomarkers, genetic panels, gut microbiome analysis. The value proposition is real. In some of these countries, the same imaging that costs $5,000 in the United States is available for $800 with shorter wait times and newer equipment. Seoul alone has built an entire medical tourism corridor around Gangnam with clinics that process hundreds of international patients per week. The risk is not the diagnostics themselves. The risk is what happens after. A finding on a scan means nothing without a physician who can interpret it, contextualize it, and manage the follow-up. A tourist who flies home with a USB drive full of imaging and no relationship with the radiologist who read it is not a patient. They are a consumer holding data they may not understand.
Level 4: Procedural tourism. The highest-risk tier. Stem cell injections or gene therapy in the Cayman Islands or Mexico. Exosome therapies in Dubai. Gene therapy in Costa Rica. Hyperbaric oxygen courses in Turkey. These are medical interventions being delivered outside the regulatory frameworks of the patient’s home country, often by providers who could not offer the same treatments at home because of local regualtions.
What the boom is getting right:
Awareness. More people are willing to travel for their health. They are thinking about preventive care or health optimization because a hotel or a clinic in another country introduced the concept. That pipeline into medicine is real.
Access. A full-body MRI in Seoul for few hundred dollars is reaching patients who would never get one at home. Diagnostic access is expanding because of tourism, not in spite of it.
Experience. Hospitality knows how to design an experience around health. Medicine historically does not. The best longevity retreats are teaching physician-led practices something about how patients want to be treated.
Competition. When a resort in Thailand offers better imaging at a third of the price, it forces domestic health systems to ask hard questions about their own pricing and access. That pressure is productive.
What the boom is getting wrong:
No continuity. A retreat lasts a week. A diagnostic trip lasts three days. A stem cell injection is a single visit. Longevity medicine is continuous. Without follow-up, without a physician who knows the patient’s history, without a plan that extends beyond checkout, these are isolated events, not medicine.
Poor regulation. Many procedural tourism destinations exist precisely because the regulations are looser. That is not always sinister, but it means the patient is bearing risk that a regulatory body would normally absorb. When something goes wrong in a stem cell clinic in an offshore jurisdiction, the recourse options are limited.
Lack of science-backed protocoles. Some of what is being sold at Level 3 and Level 4 has strong emerging evidence. Some of it has none. The patient often cannot tell the difference because the marketing is identical in both cases.
Inconsistent medical supervision. The spa with no medical director. The retreat with no physician on staff. The diagnostic clinic that hands you results with no consultation. The procedural facility where the “doctor” is a general practitioner who completed a weekend training in regenerative medicine. Medical supervision exists on a spectrum, and the lower end of that spectrum is lower than most patients realize.
What to check before you go.
Whether you are a physician advising a patient or a patient evaluating a program, these are the questions that separate serious from speculative.
Is a licensed physician supervising the program? Not advising. Not consulting. Supervising. Present. Accountable. What are their credentials, their specialty training, and their experience with the specific interventions being offered?
What are the local regulations? A stem cell therapy that is illegal in the United States is not necessarily unsafe, but the patient should understand why it is not approved at home and what evidence the destination facility is relying on instead. Ask for the published data. If there is none, that is your answer.
What does the follow-up look like? Who reads your results after you leave? Who manages an incidental finding on your MRI six months later? If the answer is “your doctor at home,” then the facility has built a product, not a care model.
What is the pricing telling you? A full-body MRI in Seoul for $800 reflects genuine cost efficiencies in the Korean healthcare system. A stem cell injection in the Caribbean for $25,000 reflects demand-based pricing for an unproven therapy with no insurance coverage. Price is information. Read it.
Is the facility transparent about outcomes? How many patients have they treated? What are the complication rates? What is the published evidence for the specific intervention you are considering? If the clinic cannot answer these questions with data, they are selling confidence, not medicine.
Is there a complaints or malpractice pathway? In your home country, a bad outcome has legal and regulatory recourse. In a medical tourism destination, that pathway may not exist. Understand what protections you have before you need them.
The Future of Longevity Tourism
The longevity tourism boom is real, it is growing, and it is not going away. The instinct behind it is good. People want to live longer and better, and they are willing to travel to do it. That same instinct sent Europeans to thermal springs for three centuries.
But the distance between a spa menu and a stem cell injection is the distance between a mineral bath and surgery. The category called “longevity tourism” now contains both, and the patient browsing options on their phone cannot always tell which is which.
Physicians belong in this conversation. Not to shut it down, but to help patients navigate the spectrum with the same rigor they would bring to any clinical decision. Ask for the evidence. Ask for the credentials. Ask for the follow-up plan. Ask who is accountable when something goes wrong.
The boom is here, let’s make is as impactful as possible for the patients.

Every week, the Longevity Docs App feels like a front-row seat to the future of medicine. Here’s what had doctors buzzing:
Midjourney’s Medical Scanner: Hype or Hardware?
Midjourney launched an ultrasound body scanner in a spa setting with cold plunges and saunas, not through radiology partnerships. The community split. “If the tech was legit and worked, why would they not want all of medicine to use it?”
A radiologist flagged the physics problem: bowel gas and bones limit what ultrasound can see. The business explanation: “They have enough capital to run it through the wellness route without needing SaMD.” The regulatory read: by not interpreting images for cancer screening, they sidestep FDA approval.
The clinical worry: “A wealthy gateway for multiple further paid investigations of benign anomalies, with a high rate of false positive, provoking anxiety and cost.” One physician reframed the whole thing: maybe the device is better suited as a therapeutic than a diagnostic.
CAC 149 in the LAD: What Would You Do Next?
Real case: 49-year-old male, ApoB treated to 75, Lp(a) under 10, clean inflammatory markers, CAC 149 with 97% in the LAD. The community said CCTA next, citing SCAPIS (n=24,791) and SCOT-HEART (low-attenuation plaque burden over 4% linked to 5-fold increase in MI). The room also broke down Cleerly (best for plaque morphology), HeartFlow (actual virtual FFR measurement), and Caristo (best perivascular inflammation analysis, not yet FDA-approved in the US). Photon-counting CT is coming but currently limited to Mayo, MGH, and NIH.
Your NAD+ Infusions Are Not Safe
A physician with 20 years of longevity practice experience posted: “Sorry guys, your NAD infusions are not safe.” Why do patients report feeling better? “The temporary release of inflammatory cytokines can feel a little like an energy rush.” The clinical reality: “For everyone who feels better for a short time, I have about 20 people who have chest pain or nausea.” A professional athlete case was shared: consistent NAD+ use during the season, surprise UCL tear, mitochondrial testing revealed fatty acid oxidation and electron transport chain dysfunction. After addressing root cause, recovery held. The takeaway: fix the mitochondria first, not force them with IV push. Some early data on oral NR for ovarian aging may tell a different story.
Stay up to date with the latest news & conversation inside longevitydocs.ai

NAD+ Supplementation Blocks Ferroptosis and Lipid Overload in Aging Cells
A new preclinical study identifies a two-pronged mechanism by which NAD+ precursor supplementation combats cellular aging: suppressing CD36-driven lipid accumulation and halting ferroptotic cell death, both of which accelerate tissue dysfunction with age. The findings are notable because ferroptosis has emerged as an underappreciated driver of organ aging, and CD36 overexpression is linked to metabolic disease and cardiovascular risk. NIH
Why it matters: Clinicians managing older patients with metabolic syndrome or cardiometabolic comorbidities should watch this pathway closely as translational work accelerates. The study adds mechanistic depth to the already crowded NAD+ supplementation field, potentially sharpening patient selection criteria for trials.
Weekend Exercise Confers Mortality Protection Rivaling Daily Physical Activity
New accelerometer-derived data show that concentrating physical activity into one or two days per week, the so-called Weekend Warrior pattern, yields substantial reductions in all-cause and cardiovascular mortality, comparable to benefits seen with distributed daily exercise. The findings carry direct clinical relevance for physicians counseling time-constrained patients, suggesting that volume and intensity may matter more than frequency.
Why it matters: This challenges longstanding public health messaging that emphasizes daily movement as the primary target. Clinicians monitoring cardiometabolic risk should consider total weekly activity load as the key prescribing metric.
Breast Tissue Epigenetic Clocks Unlock New Cancer Risk Stratification Tools
A new study demonstrates that DNA methylation-based measures of biological aging derived directly from breast tissue, not blood, carry independent predictive value for obesity-related breast cancer risk. The finding is clinically significant because it suggests tissue-specific epigenetic clocks may outperform systemic aging biomarkers in organ-level cancer surveillance.
Why it matters: Physicians managing patients with obesity and elevated cancer risk should watch for integration of these methylation panels into breast screening protocols. The research reinforces the growing case for localized epigenetic profiling as a precision oncology tool.
Elevated Tyrosine Levels Associated With Shortened Lifespan In Men
Large-scale cohort study reports that men with elevated blood tyrosine levels show reduced life expectancy, with potential loss of up to one year. Finding contrasts with branched-chain amino acid research and highlights amino acid balance—not individual amino acids—as lifespan modifier. Effect size varies by genetic background and metabolic phenotype. ScienceDaily
Why it matters: Amino acid composition, not quantity alone, predicts longevity. Tyrosine elevation may signal dysregulated catecholamine metabolism or impaired renal amino acid handling. Test comprehensive amino acid panels in male patients; consider tyrosine-to-BCAA ratio as emerging biomarker. Sex-specific effects require distinct clinical protocols.
Phosphatidylcholine Restoration Reverses Mitochondrial Aging and Cellular Energy Loss
Study identifies declining phosphatidylcholine as a primary driver of age-related mitochondrial dysfunction and ATP depletion. Researchers demonstrated that restoring phosphatidylcholine levels in aged cells restored youthful mitochondrial performance, electron transport chain activity, and cellular energy production. Finding identifies a reversible, nutrient-responsive mechanism underlying metabolic aging across tissues. ScienceDaily
Why it matters: Mitochondrial dysfunction is tractable through lipid supplementation. Phosphatidylcholine is accessible, low-cost, and shows rapid restoration of function in models. Consider phospholipid panels and targeted supplementation in patients with fatigue, cognitive decline, or metabolic dysfunction. Mechanism separates from senescence and offers layerable intervention.

Every week, I track funding, FDA approvals, product launches, and breakthrough announcements shaping longevity medicine.
TECH
Midjourney Announces New Medical Division

The first Midjourney Spa opens SF end of 2027 with the new Midjourney Scanner, a full-body Ultrasonic Computational Tomography system with 358,000 transducers, zero radiation, ~60-second scan time. Targets preventive body composition monitoring at consumer scale. Current prototype: 20-minute scan, 12 people tested, no FDA approved.
BIOTECH
Life Biosciences Doses First Patient With ER-100 Epigenetic Reprogramming Therapy

First patient dosed with ER-100, Life Biosciences' partial epigenetic reprogramming therapy for optic neuropathies (age-related vision loss and glaucoma). FDA cleared the IND in January 2026; June 2026 marks first human dosing. This is the inaugural clinical trial of a partial reprogramming approach in humans, translating years of Harvard-led research into the clinic.
BUSINESS
Winning the Longevity Market: 5 Trends Shaping the New Health Consumers

Longevity is becoming a consumer-led category in Southeast Asia, with patients acting as their own health CEOs, using wearables, digital tools, and health data to monitor themselves. Businesses across healthcare, hospitality, financial services, and consumer goods are being pushed to design for vitality, not just treatment. IPSOS
PUBLIC HEALTH
The Longevity Dividend: The Business Case for Linking Health and Wealth
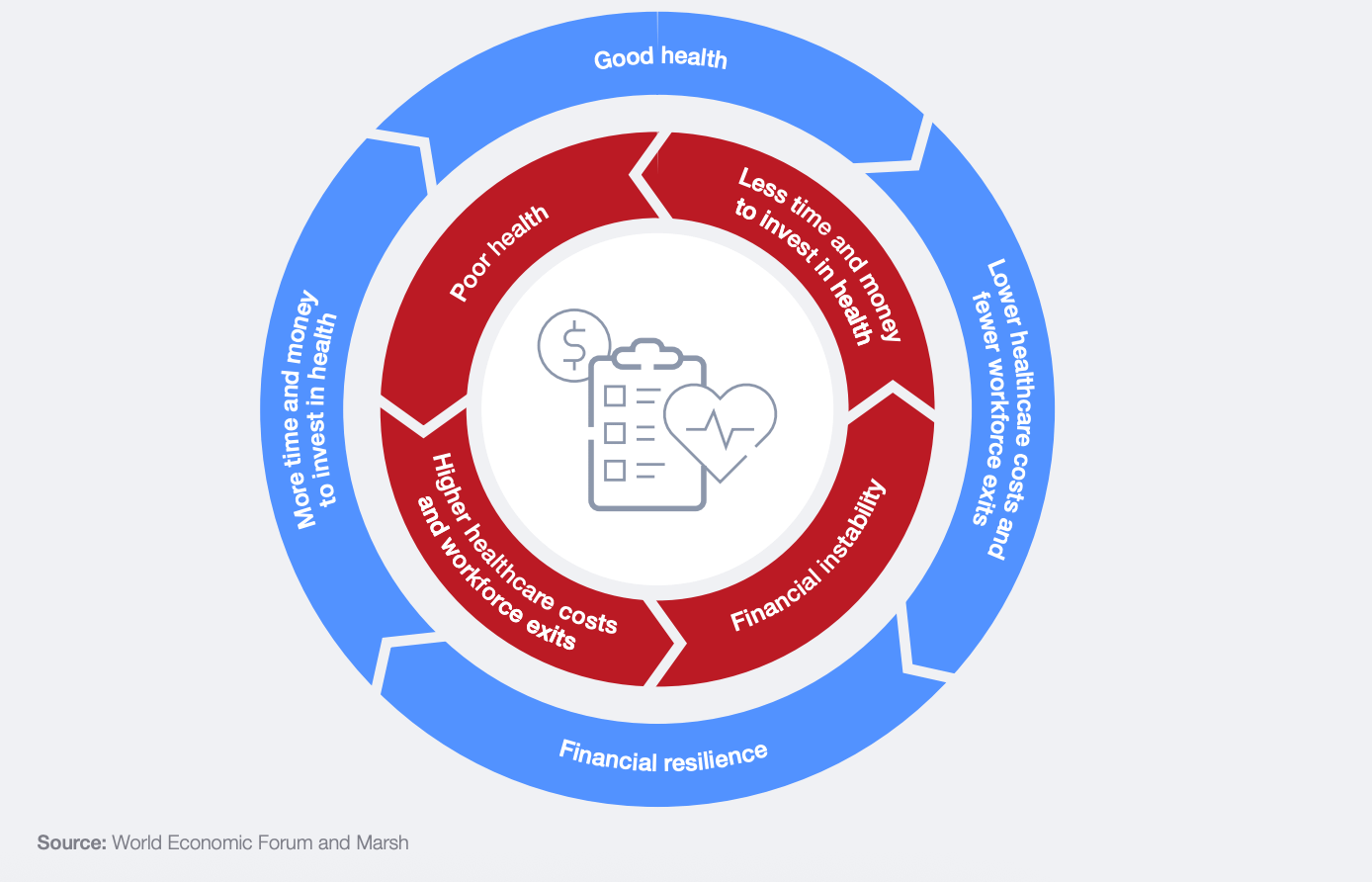
The World Economic Forum and Marsh report finds that three low-cost interventions (fall-proofing homes, increasing physical activity, expanding hearing aid access) could save healthcare systems $5.8 trillion and add $645 billion in productivity by 2040. Based on data from 21 countries, the report argues that longevity is not a problem for aging nations alone but an economic opportunity for every country on the demographic spectrum, and that physical health and financial health must be treated as one system, not two separate policy domains. WEF

Couldn’t join us in Cannes? Get the full replay of sessions, keynotes, & panels on demand.
The longevitydocs. Summit™ now lives on demand. Three days of stage time from forty-plus speakers, ready for you to watch from anywhere in the world.


The Home of Longevity Medicine
longevitydocs.™ is the largest vetted community of longevity physicians in the world, and the home of the credential that defines the field. 1,000+ doctors. 68 countries. Building the new standard of care. Every doctor should be a longevity doctor.™

Editorial Disclaimer: