

The Longevity Conference ROI: An Honest Audit
#89 Weekly Longevity Medicine Intelligence

Hey Doc,
This is Newsletter 89. I skipped a few Sundays. It is 8:38pm sunday night, docs are waiting for the newsletter. I have to ship!
Nobody warned me about this. Building a physician community is the one of the hardest thing I’ve ever done. Harder than cardiac surgery. Harder than fundraising. Harder than building companies.
Getting doctors to trust something new doesn’t happen with a marketing campaign. It happens one conversation at a time. I speak with physicians around the world every day of the week. No exception.
10 physicians to 1,000 across 68 countries in two years. The movement is real. Now we need more rooms to gather, more experiences to connect, and more role models to show what’s possible.
One mission: making longevity medicine the new standard of care. Every doctor should be a longevity doctor.
That’s what we’re building. Newsletter 89.
Dr. David Luu - Founder, longevitydocs.™

Every Wednesday, we ship something new for this community. Features, experiences, and products built by physicians, for physicians. The platform grows because you do.
Rooms - The Digital Lounge for Longevity Docs
Launching this Wednesday
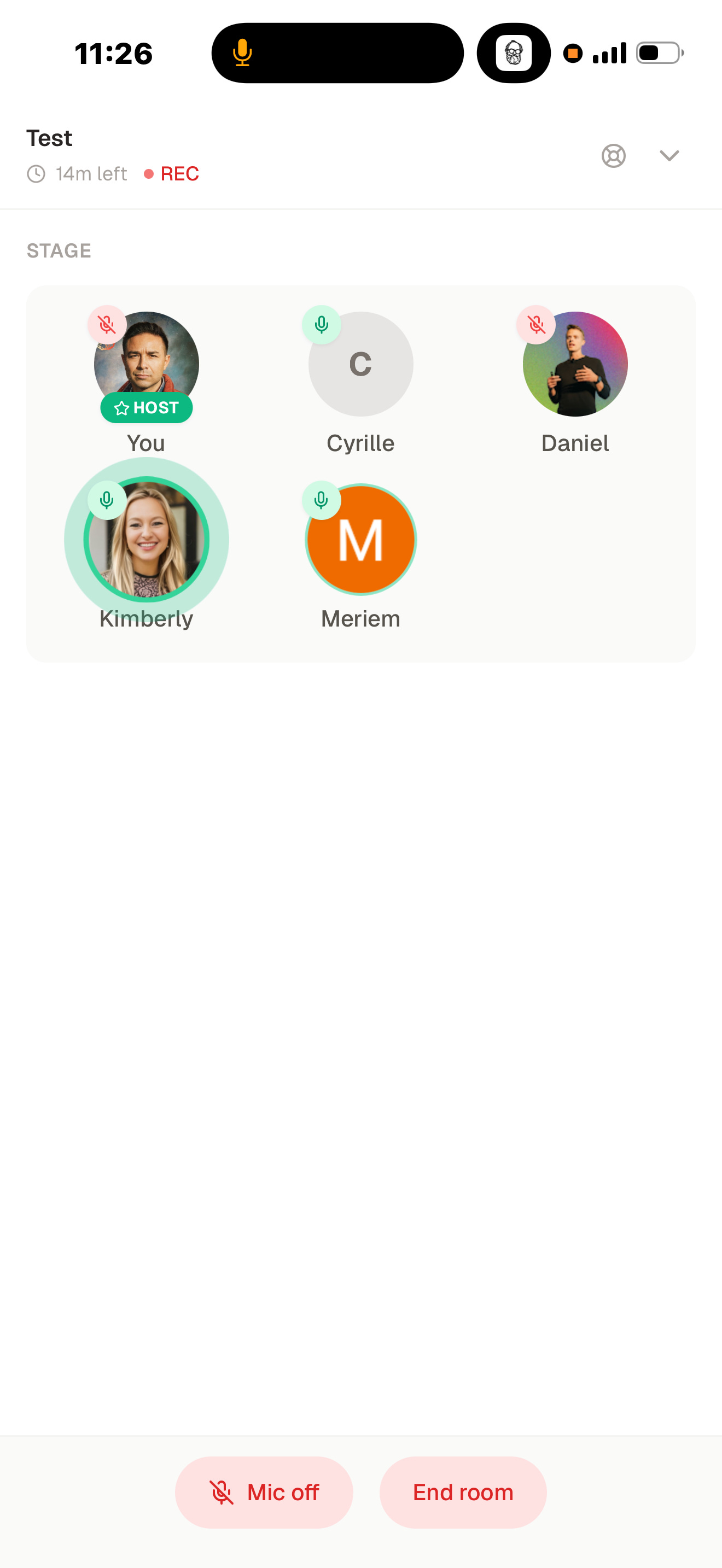
There used to be a place where doctors talked to each other. Not in a chat thread. Not on a podcast. In a room.
The hospital lounge is gone. Private practice replaced hallway conversations with isolation. The best clinical conversations you’ve had in the last year probably happened by accident, at a conference dinner, or between sessions.
We’re fixing that.
This Wednesday, we’re launching Rooms: 20-minute live audio discussions built for longevity physicians. Focused themes. Real cases. Genuine debate. Short enough to fit between patients. Deep enough to actually change how you practice.
Each week, leading physicians across the community will host sessions on clinical rounds, book clubs, practice growth, and emerging protocols. Kicking off the programming: Dr. Catherine Johnson, Dr. Mishal Reja, Dr. Omar Saleem, Dr. Jonathan Bastian, Dr. Mayoni Gooneratne, Dr. Anna Emanuel, Dr. Steve Murphy, Dr. Jila Senemar, Dr. Amanda Hill, Dr Giovanni Campanile, Dr. Sumita Jain, and more
I will open the first Room: “Do You Practice Longevity Medicine?” a live conversation on a very vibrant topic. Audio only. Physician-led. Open floor.
The lounge is back. Come in.

Each week, I try to explore one idea that could advance longevity medicine and hopefully support physicians in bringing it to life.
The Longevity Conference ROI: An Honest Audit
An honest audit of where conferences deliver and where they quietly drain you.
Sorry. This is partly our fault.
In April 2024, we organized one of the first conferences dedicated entirely to longevity medicine. Since then, the calendar has exploded. Every major city wants one. Miami. London. Dubai. Las Vegas. Cannes (our own Summit).
We helped start something. Now everyone wants in. And not all of it is good.
Some of these events are intimate, rigorous, and genuinely career-changing. Others are three days of panel discussions sponsored by energy drink brands, mattress company, wrapped around a networking dinner you didn’t need.
Your time is your most finite resource. Before you book the flight, here’s the honest audit.
5 Reasons to Attend
1. The Room Is the Product: No podcast replicates a well-curated room. The conversation that changes your practice rarely happens on stage. It happens between sessions, at dinner, in the hotel lobby. The right conference puts you in proximity to people you wouldn’t meet in five years of cold outreach.
2. Pattern Recognition at Speed: A focused conference compresses months of scattered reading into 48 hours of curated signal. You hear what’s emerging, what’s being debated, what forward-thinking physicians are actually doing in practice. Not what got published 18 months ago.
3. Clinical Confidence: Hearing a world-class clinician walk through a protocol in real time, with nuance, with pushback, with the messiness of real cases, builds a kind of confidence that a paper or course cannot replicate. That confidence changes how you show up for your patients on Monday morning.
4. Legitimacy and Visibility: Being present signals you are engaged at the frontier. For physicians building cash-pay or concierge practices, that visibility matters. Patients research their doctors. Colleagues notice who is in the room.
5. The Catalyst Effect: A partnership, a practice pivot, a collaboration, a referral network. Some of the most important decisions begin with a single conversation at a conference. You cannot predict which one. That’s an argument for being present.
5 Reasons to Think Twice
1. The Economics Rarely Add Up: Registration: $1,000 to $2,000. Flights and hotel: $1,500 to $3,000. Three days out of practice. A mid-tier conference easily crosses $5,000 to $10,000 with opportunity cost. Most physicians leave with a tote bag, a LinkedIn connection they’ll never message, and a vague intention to implement something. That is not a return. That is an expensive CME credit.
2. The Speaker Circuit Is Real: A growing number of longevity conference speakers are professional speakers first and clinicians second. Repurposed keynote. Same framework. Same book pitch. If you’ve attended more than three events in two years, you’ve almost certainly heard the content before, repackaged for a different city.
3. Sponsors Have Quietly Become the Audience Most conferences depend on sponsors, not attendees. The agenda is shaped by who is paying for it. Supplement companies, device manufacturers, and longevity tech startups are buying access to physicians.
4. The Information Is Already Everywhere The keynote will be on YouTube within a week. The panel will become a podcast. The citations will be in your inbox before you land. If information transfer is your primary reason, the conference is one of the least efficient ways to get it. The content has been commoditized. What hasn’t been commoditized is the room. But most conferences don’t deliver the room. They deliver a stage.
5. Community Without Continuity Is Just Networking The deepest failure of most conferences is what happens after. You exchanged cards. You had a great dinner conversation. You felt like you were part of something. Then you went home. And the isolation returned within a week. A conference without a living, year-round community behind it is a temporary sensation, not a structural solution to the professional loneliness that affects more physicians than the field will admit.
My personal checklist before deciding
The question isn’t whether to attend. It’s which conferences have earned your three days and your $10,000.
Before I book anything, I run through my personal checklist:
Will I learn something I don’t already know?
How fresh and relevant are the speaker perspectives or have I heard this keynote before under a different title?
Have I seen these speakers somewhere else recently (podcast, YouTube, another stage)?
Is there a real chance I’ll meet people who inspire me, challenge me, or become genuine collaborators?
Are the expo and sponsors curated or did they simply pay for a booth?
Is the format designed for conversation, not just consumption? Panels, workshops, and roundtables are not the same thing.
How many people are in the room? 2,000 attendees and 200 is a fundamentally different experience.
Is there a living community druing and after the conference?
Do I know anyone going? A warm room accelerates everything.
Is the city worth the trip? That counts too. Where you land shapes how open you are to everything that follows.
10 yes answers: block the calendar. Fewer than six: wait for the recap.
PS: Full disclosure - Longevitydocs organizes its own conferences. And yes, we try to check all ten boxes. You can hold us to it. Cannes, June 9–11.

Every week, the Longevity Docs Chat feels like a front-row seat to the future of medicine. Here’s what had doctors buzzing:
GLP-1 & Hair Loss
A physician shared a patient with prior severe hair loss who did well for ~8 weeks on re-challenge with tirzepatide. Now reporting scalp tingling and early shedding. Continue? Stop? Dose adjust?
The first wave of responses pointed to the well-established indirect mechanism:
“It’s not a direct result of the med. It’s rapid weight loss changes, similar to bariatric. People under-eat and get nutritional deficiencies. Low protein plus low ferritin/zinc → hair shedding.”
The consensus here: check ferritin, albumin, zinc, B12, thyroid. Go low and slow. Replenish. Hair comes back.
Then a dermatologist pushed back and the thread shifted:
“Women are 15–17x more likely to experience it. There is a theory GLP-1 is activating adipocyte-derived stem cells leading to inflammation and accelerated skin and scalp aging. Although most experts say it’s indirect, clinically I’m seeing something more in some patients. I just don’t know how to identify them before.”
Another member flagged a key co-mechanism:
“TE can unmask AGA in certain patients. I wonder if that’s happening in a subset of the hair loss we’re seeing.”
The dermatologist shared her full GLP-1 Hair Loss Physician Protocol. Within minutes, the requests flooded in from across the group. Her core philosophy:
“Remove the inflammatory triggers in personal care products first: sulfates, phthalates, preservatives are causing inflammation and making things worse. These patients are desperate so they are using all kinds of crazy things on their scalp. Less is more.”
On supplements:
“I don’t use the off-the-shelf hair loss supplements. I use targeted, personalized supplementation. Don’t need biotin in crazy amounts.”
What’s next
A dedicated Longevitydocs Room on GLP-1 and hair loss is being planned. Audio only, physician-led, open discussion. Stay tuned for the date.
“Hair is never just one thing.”

GLP-1RA and the possible skin aging
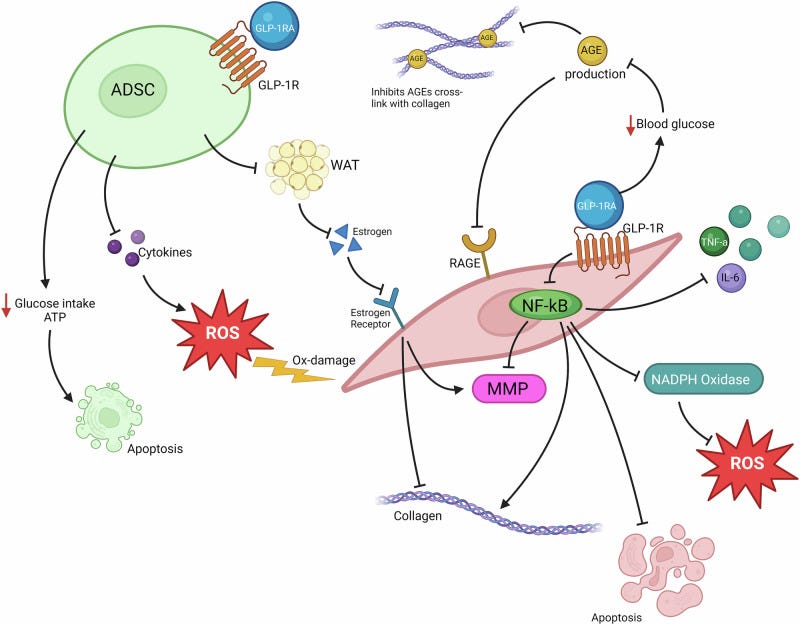
GLP-1 drugs (Ozempic, Wegovy, Zepbound) are triggering “Ozempic face” through four mechanisms: disrupting adipose-derived stem cells, reducing estrogen production in the skin, starving skin cells of energy, and accelerating collagen breakdown. It’s not just fat loss, there’s direct biological aging happening at the cellular level.
The twist: the same drugs reduce AGEs and systemic inflammation, which protects skin health. Two opposing mechanisms, same drug. Endocrine
Why it matters for physicians: What your patients are seeing in the mirror is real biology, not vanity. Screening for skin aging markers before and during GLP-1 therapy may become standard of care, and the dermatology-longevity overlap is wide open for clinical leadership.
Dasatinib + Quercetin Causes Demyelination in Mices
The popular senolytic combo D+Q (currently in multiple clinical trials) caused significant white matter damage in both young and old healthy mice. Oligodendrocytes (the cells that produce myelin) stopped functioning properly without actually dying, triggered by endoplasmic reticulum stress and the unfolded protein response.
Why it matters for physicians: D+Q is being prescribed and self-administered widely in longevity medicine. This study suggests neurological risk may exist even in healthy individuals, at any age. Clinical trials haven’t been designed to catch this. Until human data clarifies the risk, caution is warranted.
Molecular Evolution of Animal Aging
 interacting with the environment (blue oval).")
Nature has solved longevity many times over. Long-lived species (bowhead whales, bats, axolotls, naked mole-rats) share four common strategies: superior DNA repair, controlled inflammation, sustained regenerative capacity, and environmental resilience.
The most clinically actionable findings:
Inhibiting the enzyme 15-PGDH restores muscle strength by 10–15% in aged mice within one month — and also protects against Alzheimer’s
DNA double-strand break repair is the strongest molecular predictor of lifespan across species — and can be pharmacologically boosted
Senolytic precision matters — some senescent cells are protective; removing all of them causes harm
Gut bacteria drive immune aging through a microbiome-senescence feedback loop that’s potentially reversible
Why it matters: The biology of extreme longevity already exists in nature. The clinical opportunity is learning to replicate it — selectively, safely, and measurably.

Welcoming the Certified Longevitydocs Candidates
This week, three physicians from across the world made the decision. They just joined our Certified LongevityDocs program to earn their CLD certification. Different specialties. One decision.



Dr. Samireh Said is a double board-certified dermatologist with 33 years of experience, trained at the University of California Irvine. After decades of treating skin at the surface, she's now building the clinical framework to treat it at the root: through the lens of aging biology. She joins the CLD program to formalize what she's already seeing in her practice: longevity medicine and dermatology are the same conversation.
Dr Daniel Kessler is double board-certified in Family Medicine and Integrative Holistic Medicine, trained at Emory, with two years at the CDC researching environmental toxins and additional training at the Mayo Clinic. He founded the KADAN Institute when conventional care reached its ceiling. He joins the CLD program to build the evidence layer his root-cause practice has always needed.
Dr. Bryan Love is a Fellow of the American College of Surgeons, trained at Lewis Katz School of Medicine at Temple University, with a career spent at the sharpest edge of human physiology — keeping people alive under the most extreme conditions. He joins the CLD program because the next frontier isn't the trauma bay. It's what happens before patients ever get there.
Three different entry points. One direction. Get certified.

Every week, I track funding, FDA approvals, product launches, and breakthrough announcements shaping longevity medicine.
AI & TECH
Epic launches real-time disease surveillance across 300M patient records

Epic has quietly deployed one of the most powerful disease surveillance systems in medicine. Using its Cosmos platform — 300 million patient records across 2,067 hospitals — it now monitors county-level diagnosis rates and issues public alerts when illness rates spike beyond statistical norms. The system has already flagged elevated rates of bronchiolitis, measles, strep, and viral gastroenteritis across multiple states. Alerts are clinician-reviewed before publication and use the Farrington algorithm, the gold standard in public health surveillance, to filter seasonal noise.
Why it matters for longevitydocs: Real-world surveillance at this scale changes the signal-to-noise ratio in population health. For longevity practices tracking systemic inflammation and immune resilience, this kind of longitudinal signal infrastructure is what evidence-based prevention has always needed.
RESEARCH
Nestlé enters the longevity science space

Nestlé and Nanyang Technological University Singapore are launching a multi-year joint research lab focused on targeted nutrition and biological aging. The collaboration will study metabolic health, mobility, sleep, and menopause — combining Nestlé’s global R&D infrastructure with NTU’s clinical research capabilities. The move signals that food companies are formally entering the longevity science space, not as sponsors, but as investigators.
Why it matters for longevitydocs: When Nestlé funds aging research, the field has crossed a commercial inflection point. The nutrition-longevity connection is becoming investable science — and physicians who understand this space will be positioned ahead of the partnerships that follow.
CULTURE
America is structurally unprepared for its own longevity crisis

In 2026, the oldest Baby Boomers turn 80. Roughly 80% of households with adults aged 60+ lack resources for long-term care. Fewer than 5% of U.S. homes have basic accessibility features. The healthspan-lifespan gap currently sits at 12.4 years. It means most Americans spend over a decade in poor health before death. Researchers are calling for longevity preparedness to replace retirement planning as the organizing framework for aging policy.
Why it matters for longevitydocs: This is the demand signal your practice exists to meet. The gap between what the system offers and what patients actually need is where longevity medicine lives, and it is only widening.

Mastermind Replays Now Available
3 Masterminds. 3 topics reshaping longevity practice: AI & Tech, Peptides, and Hormones - featuring the dozens of faculty. Trusted by hundreds of physicians
If you weren’t in the room, this is your second chance.

Conferences
Jun 9–11 — Longevity Docs Cannes 2026”: Awards & Summit
Jun 29–Jul 1 — A4LI H-SPAN Summit · Washington, DC Longevity medicine meets regulation and policy.
Aug 24–28 — ARDD · Boston Where aging research meets drug discovery.
Oct 17 — Longevity Docs Skin Longevity Mastermind · New York, NY. Curated physicians. Deep science. One room.
TBA — Longevity Clinics Roundtables · Buck Institute Clinical practice meets research infrastructure.

The Home of Longevity Medicine
longevitydocs.™ is the world’s leading longevity physician community - 600+ doctors across 50 countries united by a single conviction: every doctor should be a longevity doctor. Founded by Dr. David Luu, the platform offers its members network, education, and experience with the mission to democratize longevity medicine.
Not a member yet? Join longevitydocs™
We’re a physician-only network. Curated. Vetted. Built on trust. If you’re committed to practicing longevity medicine with rigor, peer support, and shared standards → this is your community. Apply to connect with our team.
Longevity medicine is the personalized, evidence-based practice of modifying the root mechanisms of aging (biological, cognitive, and psychosocial) before they become disease, extending healthspan, not just lifespan. Using advanced diagnostics, precision interventions, and AI-enabled monitoring, it translates measurement into action across every medical discipline. Success is measured in functional capacity, vitality, and disease-free years.

Subscribe to the Longevity Docs Newsletter
Longevity medicine is moving fast. Every week, we bring you what matters: clinical insights, research signals, and perspectives from 600+ physicians across 50+ countries. One newsletter. Built for the physicians shaping this field.
Editorial Disclaimer:
Good discussion of the ROI on conferences!