

The Longevity Clinic Gold Rush
#86 Weekly Longevity Medicine Intelligence

Hey Doc,
I just got back from disappearing. This is Sunday! I landed at JFK at 11:29pm last night. One week. No meetings. No agenda. No Zoom. Just me and one question I needed to answer.
I call it Architect Week. Once a quarter, I disappear. Not to rest but to think. The kind of thinking that’s impossible when the calendar is full and the notifications are on. The kind that only happens when you remove everything competing for your attention.
This quarter the question was this: How do we help physicians build the longevity practice they went to medical school to build
I think I found the answer.
It’s not a framework, courses, or protocols. It’s The Operating System, built specifically for physicians who’ve decided that fighting aging is the most important work medicine can do right now.
In the meantime… if you haven’t tried it, consider your own Architect Week. Pick a place or stay home. Clear your calendar. Choose one question. Sit with it until something breaks open.
What would would your question? Respond to this newsletter, I read every single one.
Dr. David Luu - Founder, longevitydocs.™


Each week, I try to explore one idea that could advance longevity medicine and hopefully support physicians in bringing it to life.
The Longevity Clinic Gold Rush: 5 Pros, 5 Cons
In 2020, longevity clinics were a niche experiment. In 2026, they are a global industry.
Serotonin Centers crossed 100 franchise locations inside gyms. Next Health sold 50+ territories. Fountain Life raised $108M. SHA and Clinique La Prairie are expanding into Asia and the Middle East. Neko Health is making it accessible at scale.
But the stronger signal isn’t the startups. It’s the institutions.
Weill Cornell launched a 12-month Longevity Medicine Program. Northwestern opened the Human Longevity Clinic. Mayo Clinic is building its own program. Sheba Medical Center became the world’s first academic institution with a dedicated longevity center. Abu Dhabi created the first government regulatory framework for longevity medicine on the planet.
When governments regulate and medical schools curriculum, a field has arrived.
$8.5 billion deployed in 2024 across 325 deals. Average deal size jumped from $20M to $69M. UBS projects $8 trillion by 2030. Over 800 longevity clinics operating in the US alone.
This is no longer about who opens the nicest clinic. This is about who sets the standard, and who gets left behind when it’s set without them.
And with that shift come major opportunities and serious challenges.
5 Pros
1. Patients are already here. They walk in with Function results, Oura scores, and biological age reports they have already GPTed. Educated, motivated, and paying cash, the demand is not something you need to create.
2. Cash-pay finally works as a business model. Memberships, annual panels, and protocols built around outcomes rather than billing codes. No prior authorizations, no insurance battles, just a practice that gets paid to deliver results.
3. Standards are being written right now, with or without you. Weill Cornell, Northwestern, Mayo, and Sheba are building longevity programs because the demand justifies it. Physicians who engage now help shape the standards
4. Science has never been more actionable. GLP-1 beyond weight loss, multi-omics clocks, AI, senolytics, the research moves every month and the tools to apply it now exist outside of research institutions.
5. Tools are within reach of every serious clinic. Genomic sequencing, liquid biopsies, AI imaging, and continuous biomarker monitoring are now available at the individual clinic level. The gap between what is possible and what most physicians offer has never been wider.
5 Cons
1. Anyone can open a longevity clinic. MedSpas are rebranding, gyms are adding IV drips, and HNWI are opening clinics like passion projects. Patients will look for trusted partner and real clinical care.
2. Training gaps are a patient safety problem. Less than 1% of medical school hours cover nutrition. Zero cover longevity medicine. Physicians opening clinics with enthusiasm but no foundation are not practicing longevity medicine.
3. Patient acquisition has become a war of budgets. Paid digital is saturating fast. Word of mouth does not scale. The clinics winning on acquisition are spending at levels most independent physicians simply cannot match.
4. Outcomes data does not exist, and that grace period is ending. Every clinic promises biological age reversal and optimized biomarkers. Almost none can prove it with publication. Patients and regulators will start demanding evidence.
5. Regulatory scrutiny is arriving faster than most physicians realize. Peptides, compounding pharmacies, CLIA certification, marketing claims, the FDA has already issued warning letters. When the first serious adverse event hits a franchise location, the response will be swift and broad. Build on solid ground now or scramble to retrofit it later.
The Opportunity
There is a white space in this market that almost nobody is talking about.
On one side, you have capital intensive brick and mortar clinics spending millions on real estate, equipment, and overhead before seeing their first patient. On the other, digital platforms with no physicians, no clinical judgment, and no accountability for what happens when the protocol does not work. In between, concierge medicine practices with loyal patient bases but zero longevity expertise, and no roadmap to build it.
None of them is what the market actually needs.
What the market needs is the longevity physician who owns and runs their own practice, serves up to 400 carefully selected patients, operates with a small focused team, and builds something that no platform or franchise can replicate: a real clinical relationship, grounded in evidence, tracked with outcomes data, and scaled with the right tools.
This physician educates their patients continuously. They publish their outcomes. They participate in a global peer network that keeps their protocols sharp. They use AI to scale their attention without diluting their judgment. They do not compete on price because they do not need to. They compete on results.
That position is still wide open.
The institutions are building. The governments are regulating. The franchises are scaling. And in the middle of all of it, there is room for the physician who simply decides to do this right.
The only variable left is you.

Every week, the Longevity Docs WhatsApp group feels like a front-row seat to the future of medicine. Here’s what had doctors buzzing:
The questions we are still asking
Every week I try to summarize the best discussions and topics worth reading about from our physician community. This week I want to take a different approach: less about what we know, more about what we don’t. These are the questions your colleagues are actively debating, and the honest answer to each one is: we are not there yet.
Does spermidine promote cancer growth?
A new paper surfaced a potential mechanism linking spermidine, one of the most popular anti-aging supplements, to cancer cell proliferation. The group flagged it immediately. The pattern is familiar: a compelling mechanism, promising observational data, then an RCT or mechanistic study that complicates the picture. Antioxidant vitamins showed strong early promise before large trials returned mostly neutral or harmful signals. Metformin followed a similar arc for cancer prevention. The honest position right now: spermidine’s longevity benefits may be real, but we do not yet know whether the same pathways that promote autophagy could also accelerate tumor growth in susceptible individuals.
Is HRV becoming a moral compass rather than a clinical metric?
One member put it bluntly: “HRV is now less a metric than a moral compass, encouraging us all to drink less, inhale more, fetishise recovery and treat a late night like an act of self-sabotage.” The clinical question underneath is serious. Are we tracking HRV because it improves outcomes, or because patients and physicians find it emotionally compelling? Goodhart’s Law applies here: when a measure becomes a target, it ceases to be a good measure. Morning HRV and nighttime HRV measure different things. The goal is stress tolerance, not a better number on a ring.
Proceed with nuance. HRV is a useful signal. But conflating the metric with the outcome is a trap worth naming explicitly with patients.
How do you actually measure senescent cell load in a clinical setting?
The question came up in two parts: how do you determine the indication for senolytics, and how do you measure whether they worked? There is no validated, widely accessible clinical assay for senescent burden. p16, p21, and SA-beta-galactosidase exist in research settings. Circulating SASP markers such as IL-6, IL-8, and GDF-15 are used as proxies. But a clean, reproducible clinical tool for tracking senolytic response does not yet exist in the way we track LDL after a statin.
Even among the world’s leading longevity physicians, this question has no clean answer.


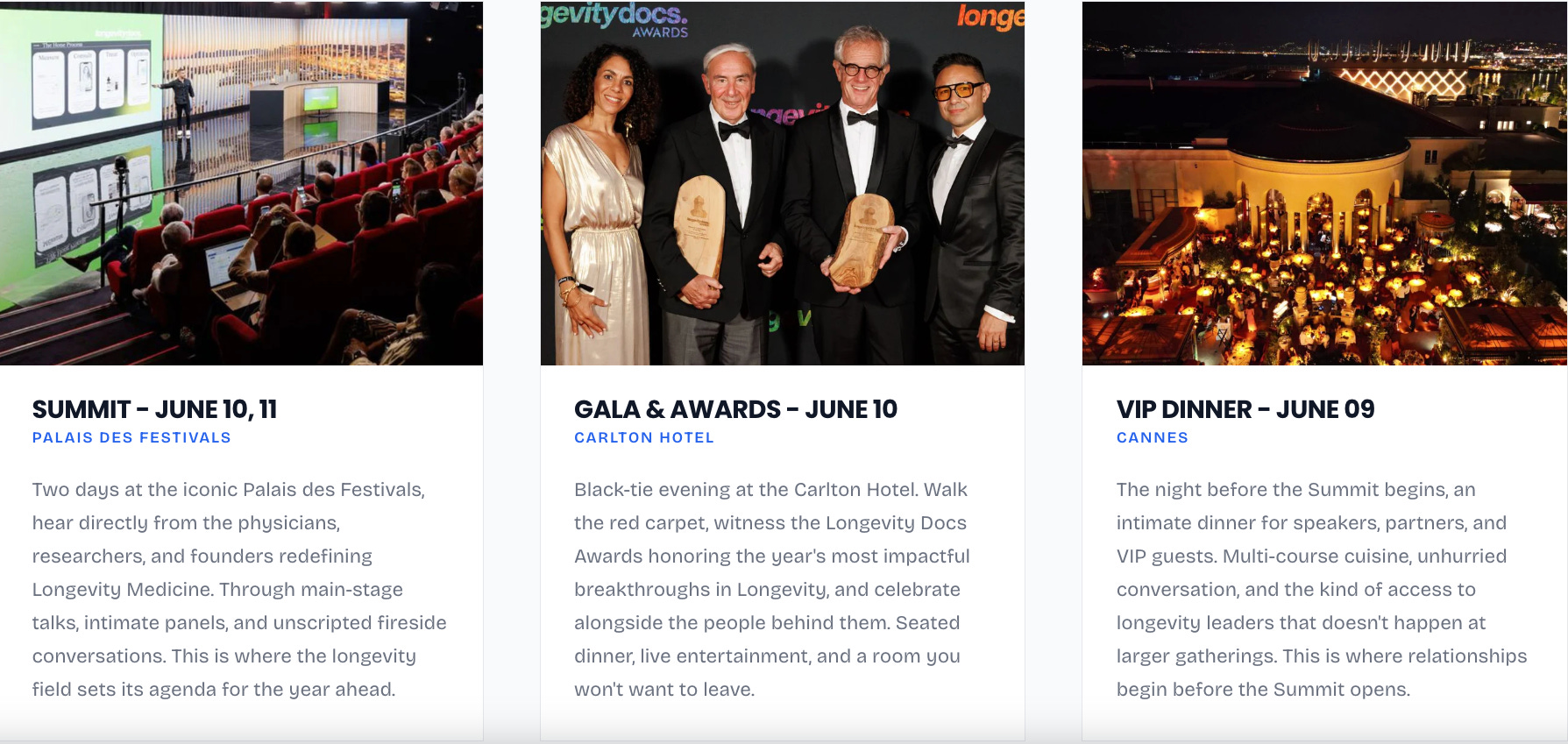
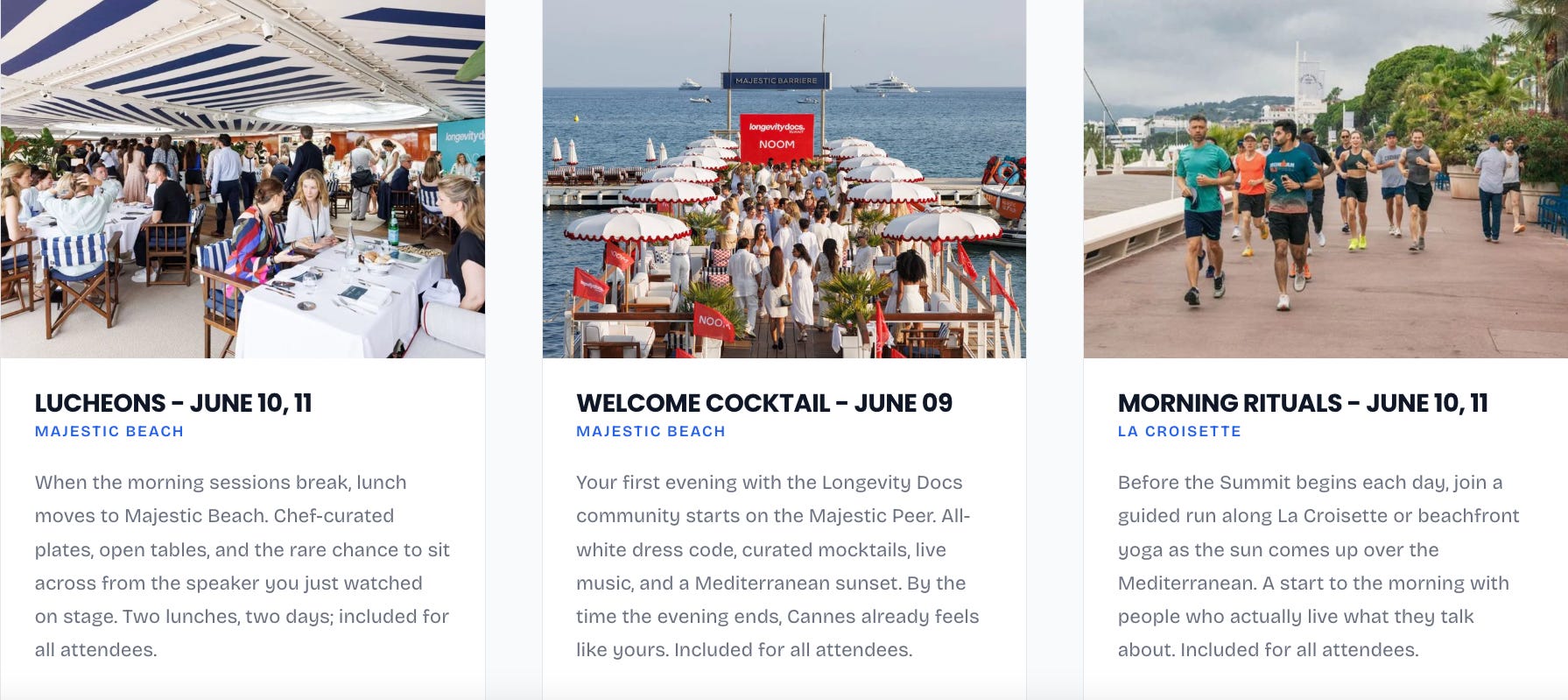
Last June, physicians, researchers, and founders from around the wordl gathered in Cannes for two days.
Watched the Mediterranean turn gold from the Majestic Pier. We ran La Croisette at sunrise. Had lunch with speakers on the beach. We left with protocols, partnerships, and friendships that don’t happen at any other event in medicine.
That was year one. This is year two, and it’s not slowing down.
The longevitydocs Summit & Awards is becoming the most important gathering in longevity medicine. Not because of the venue. Because of what happens when the right physicians and partners are together in the same room.
June 9–11. Cannes. You should be there.
Passes increase on March 29th.

Your brain talks to your skin, and stress is the messenger
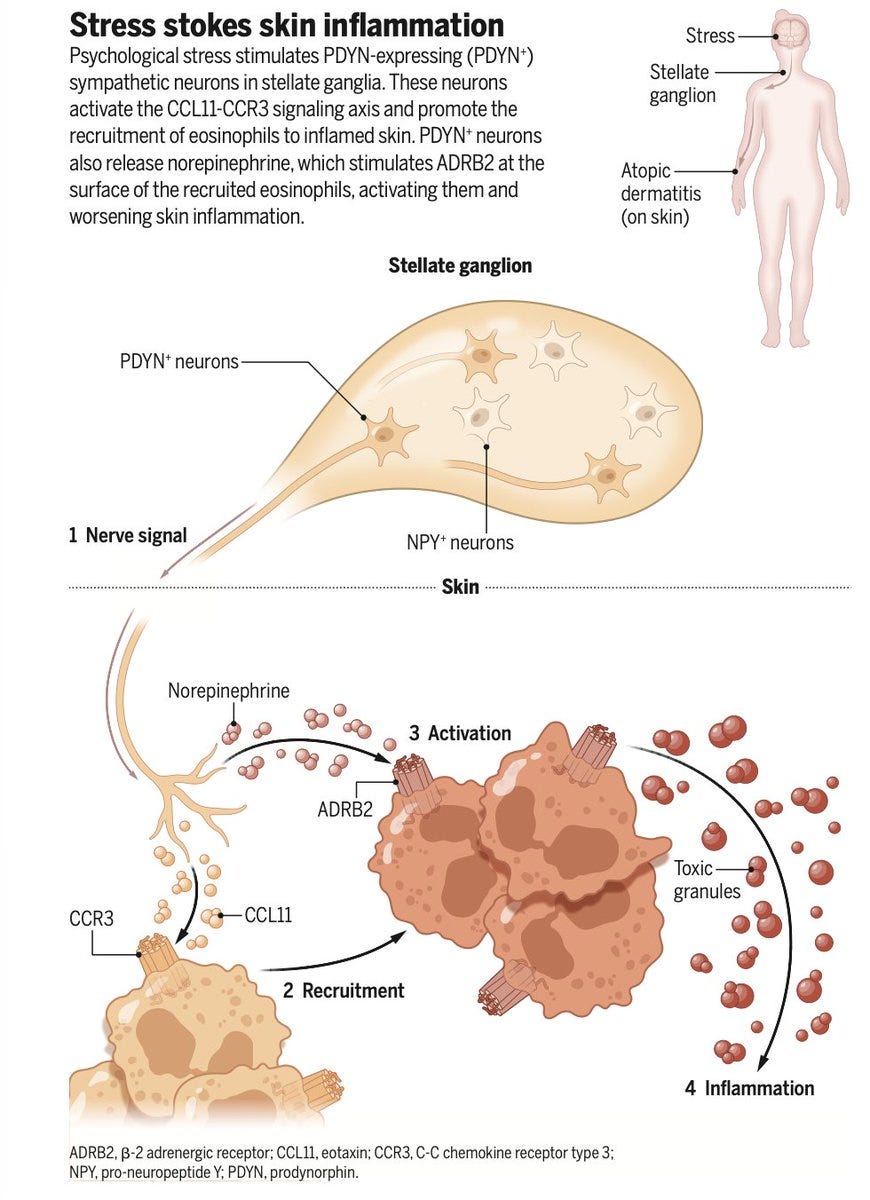
A new study identified a specific population of norepinephrine-producing sympathetic neurons that directly innervate the skin and drive stress-induced flares of atopic dermatitis in mice via an eosinophil-dependent pathway. This is the first dedicated neuroimmune axis mapped between psychological stress and skin inflammation at this level of precision — and it opens the door to targeted interventions that block the neural pathway rather than broadly suppressing the immune response. For physicians managing patients with stress-related skin conditions, "reduce stress" is finally getting a clinical mechanism behind it. Science
Four biomarkers to predict heart disease before it starts.
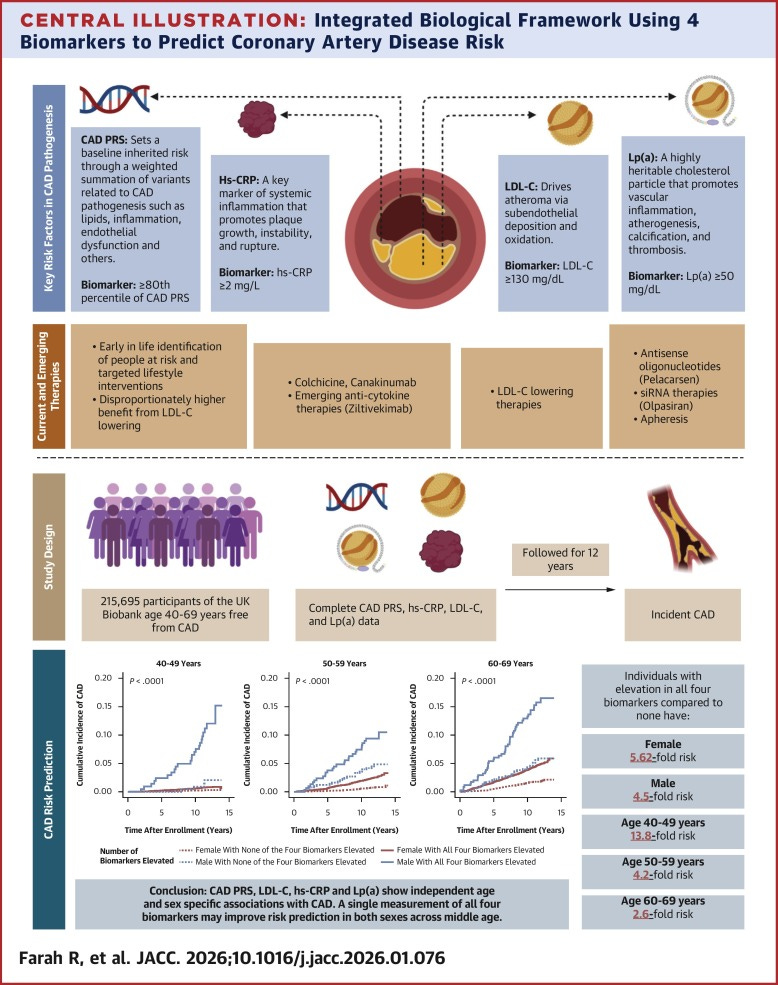
A JACC study found that a single midlife measurement of CAD polygenic risk score, hsCRP, LDL-C, and Lp(a) predicts future coronary artery disease across both sexes and ages 40 to 69. It matches traditional clinical risk calculators while catching patients those calculators miss entirely. Most of your patients walk in with at least two of these already run. This gives you clinical justification to systematize all four as a standard longevity panel at first visit, especially in patients in their 40s where biomarker-based screening outperforms conventional tools the most. JACC
Epigenetic clocks changes predict long-term mortality
Multiple epigenetic clocks have been developed to quantify biological aging. However, whether longitudinal changes in epigenetic clocks carry independent information on health and survival has remained uncertain. Here, we show that longitudinal changes in several epigenetic clocks are independently associated with long-term mortality in a cohort that was followed for up to 24 years. Nature Aging
Real-world clinical utility of tumor whole-genome sequencing in solid cancers
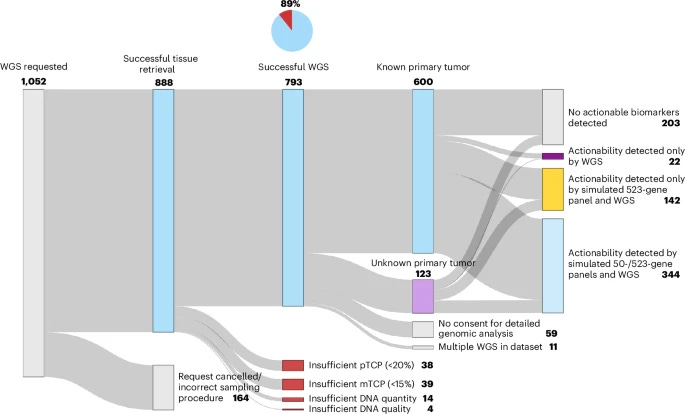
In a real-world study of 888 solid cancer patients, whole-genome sequencing (WGS) succeeded in 89% of cases with a median turnaround of 6 working days, identifying actionable biomarkers in 73% of patients. Those who received biomarker-informed treatment lived a median of 96 days longer than those who did not. WGS was especially impactful in cancers of unknown primary, contributing to diagnosis or treatment options in 67% of cases. Overall, WGS-based diagnostics had meaningful clinical consequences for 41% of all patients tested, making a strong case for its routine use in oncology. Nature Medicine

Every week, I track funding, FDA approvals, product launches, and breakthrough announcements shaping longevity medicine.
CARE
Costco enters fertility care

As part of a monthly membership agreement, Costco members gain immediate access to Sesame fertility care coordination, complete diagnostic workups, and a clear path to specialty treatment. With a universal intake policy, every patient starts with Sesame and receives a comprehensive intake evaluation, coordinated diagnostic support, and a referral to highly-experienced specialty care with IVI RMA North America when clinically appropriate. Patients arrive at IVI RMA North America clinics informed, prepared, and ready to focus on personalized fertility planning and treatment.
───
AI
Perplexity launches a consumer health AI that connects EHR and wearable data

Perplexity, best known as an AI-powered search engine, has moved into consumer health with a dedicated tool designed to link electronic health records and wearable device data into a unified AI interface. The product is positioned as a personal health intelligence layer, allowing patients to query and interpret their own clinical and biometric data through a conversational interface. Modern Healthcare
───
SCIENCE
This overlooked organ may be more vital for longevity than scientists realized

In one study published on Wednesday in the journal Nature, researchers used artificial intelligence to analyze around 27,000 patient computed tomography (CT) scans and medical records to reveal that the health of the thymus may be linked to whether an individual develops cardiovascular disease or lung cancer or dies from any cause.
───
WEARABLES
A biotech turns to Apple Watch to study its Parkinson’s drug

PHARMA/BIOTECH
Lilly finds a hidden chemical reaction in compounded tirzepatide with B12
Testing across ten compounded tirzepatide samples obtained from pharmacies, medspas, and telehealth platforms found a previously unknown impurity in all of them. The impurity results from a direct chemical reaction between tirzepatide and vitamin B12, including methylcobalamin, hydroxocobalamin, and cyanocobalamin. Fierce Pharma

Mastermind Replays Now Available
3 Masterminds. 3 topics reshaping longevity practice: AI & Tech, Peptides, and Hormones - featuring the dozens of faculty. Trusted by hundreds of physicians
If you weren’t in the room, this is your second chance.

Conferences
Jun 9–11 — Longevity Docs Cannes 2026”: Awards & Summit
Jun 29–Jul 1 — A4LI H-SPAN Summit · Washington, DC Longevity medicine meets regulation and policy.
Aug 24–28 — ARDD · Copenhagen, Denmark Where aging research meets drug discovery.
Oct 17 — Longevity Docs Skin Longevity Mastermind · New York, NY. Curated physicians. Deep science. One room.
TBA — Longevity Clinics Roundtables · Buck Institute Clinical practice meets research infrastructure.

The Home of Longevity Medicine
longevitydocs.™ is the world’s leading longevity physician community - 600+ doctors across 50 countries united by a single conviction: every doctor should be a longevity doctor. Founded by Dr. David Luu, the platform offers its members network, education, and experience with the mission to democratize longevity medicine.
Not a member yet? Join longevitydocs™
We’re a physician-only network. Curated. Vetted. Built on trust. If you’re committed to practicing longevity medicine with rigor, peer support, and shared standards → this is your community. Apply to connect with our team.
Longevity medicine is the personalized, evidence-based practice of modifying the root mechanisms of aging (biological, cognitive, and psychosocial) before they become disease, extending healthspan, not just lifespan. Using advanced diagnostics, precision interventions, and AI-enabled monitoring, it translates measurement into action across every medical discipline. Success is measured in functional capacity, vitality, and disease-free years.

Subscribe to the Longevity Docs Newsletter
Longevity medicine is moving fast. Every week, we bring you what matters: clinical insights, research signals, and perspectives from 600+ physicians across 50+ countries. One newsletter. Built for the physicians shaping this field.
Editorial Disclaimer:
Strong framing. The line that stayed with me is not that longevity is booming, but that standards are being written in real time by whoever can combine evidence, operations, and restraint, and medicine has never exactly suffered from too little ambition. Very astute.
Very interesting read, thanks doc