

The Biomarker Gold Rush
Issue 72: The front page of longevity medicine - curated by doctors, for doctors.


Hey Doc,
The Longevity Medicine has reached an inflection point.
Function raised $298M at a $2.5B valuation, offering labs for $1/day.
Hims launched 120-biomarker panels.
This isn’t news. It’s validation. Investors are betting billions that comprehensive biomarker testing will become as routine as an annual checkup, and they’re right. In five years, 150–200 biomarkers per person will be normal.
But here’s the truth: Consumer platforms can democratize testing. They cannot democratize outcomes.
Function can generate 50 million lab results. What they can’t generate is 50 million patients with extended healthspan. That gap between data and outcomes is where longevity medicine lives.
And the technology accelerating this gap is moving faster than the infrastructure to support it: proteomics, AI-derived biomarkers, multi-omics integration…
We can measure aging.
We’re still building the system to act on it.
Three questions now define the future:
What is the role of longevity physicians when AI interprets biomarkers?
Does access to data improve outcomes or just create anxiety?
Will tech platforms become unregulated health systems if doctors don’t lead?
Big announcement coming soon!
Healthy Sunday!
Dr. David Luu - Founder, longevitydocs.™
longevitydocs.™ is the world’s largest physician network in longevity medicine, serving 600+ vetted physicians across 50+ countries. We unite physicians, industry, and institutions to build the trusted global infrastructure that makes longevity medicine the new standard of care.
Longevity medicine is the personalized, evidence-based practice of modifying the root mechanisms of aging (biological, cognitive, and psychosocial) before they become disease, extending healthspan, not just lifespan. Using advanced diagnostics, precision interventions, and AI-enabled monitoring, it translates measurement into action across every medical discipline. Success is measured in functional capacity, vitality, and disease-free years.

Each week, I try to explore one idea that could advance longevity medicine and hopefully support physicians in bringing it to life.
The Biomarker Gold Rush: 5 Pros, 5 Cons
A $2.5B valuation just redefined the diagnostics landscape.
Function Health raised $298M, dropped membership to $365/year, and launched Medical Intelligence Lab: an AI engine merging 160+ biomarkers, full-body imaging, wearables, and medical records into personalized protocols.
Hims & Hers countered with Labs: 120 biomarkers, app-based results, doctor-developed action plans at a fraction of traditional costs.
Oura is layering biomarkers onto continuous monitoring. VCs are pouring billions into the infrastructure.
This is no longer about who runs the best labs. This is about who owns the intelligence layer for human health.
And with that shift come major opportunities and serious risks.
5 Pros
1. Biomarker literacy goes mainstream: Millions of people will now understand ApoB, Lp(a), inflammation markers, VO2, sleep metrics, and biological age. This raises the baseline for every clinic.
2. More patients arrive “pre-worked up”: 160+ biomarkers already measured → less guesswork → more time focused on intervention and prevention.
3. Demand for longevity medicine explodes: When patients get dashboards, they want interpretation, protocols, and outcomes. They don’t want data—they want physicians trained in longevity medicine who can translate data into extended healthspan.
4. Multi-omics becomes accessible: Genomics, epigenetics, AI-imaging, what was once academic now reaches the consumer layer, accelerating adoption in clinical practice.
5. The category gets validated: Investors and public markets are saying the same thing we’ve said for years: Precision, preventive, longevity medicine is the future of healthcare.
5 Cons
1. Data without clinical context = anxiety: DTC platforms give signals, not answers. Without physicians, biomarkers turn into worry, not prevention.
2. Patients arrive with AI-generated protocols: Some helpful. Some misleading. Not personalized. All require expert correction, which increases clinical burden.
3. No DTC platform can deliver medical-grade care: They can’t diagnose nuance, manage risk, order advanced diagnostics, or run specialist networks. That still falls on physicians.
4. Validation risk is real: AI biomarkers must meet regulatory standards (EBAI, FDA, etc.). If tools misclassify risk or miss disease, liability shifts back to the clinician.
5. Unregulated “pseudo-health systems” may emerge: If physicians don’t lead, tech platforms could become de facto health ecosystems, without clinical oversight, outcomes tracking, or standards.
The Opportunity
Consumer platforms are building the front door to longevity.
Longevity physicians can own the destination.
Patients will get labs anywhere.
But they will need:
Advanced interpretation
Real protocols
Specialist input
Clinical oversight
Outcomes
Biomarkers are becoming universal.
Clinical judgment is becoming scarce.
The biomarker gold rush won’t be won by who tests fastest.
They’ll be won by who delivers outcomes.

Every week, the Longevity Docs WhatsApp group feels like a front-row seat to the future of medicine. Here’s what had doctors buzzing:
Brain White Matter Lesions in Perimenopausal Women
A physician asked about brain MRI reports dismissing white matter hyperintensities as “not clinically significant, likely age-related, often seen in headache sufferers.” What are others seeing?
What followed proved why physician networks are essential
The Neurologist explained why radiologists’ liability-driven reports miss clinical reality: “A 75-year-old with moderate burden is different from a 30-year-old with migraines. The canned reading isn’t helpful. These lesions often reflect poor brain vascular irrigation, we need to address blood flow, glycocalyx health, and mitochondrial function.”
The Radiologist confirmed the limitation: “Radiology shows anatomy, not function. I have to guess the history because scans don’t tell me the cause. While most are from hypertension and small-vessel disease in people over 50, the differential explodes when patterns don’t fit: MS, vasculitis, Lyme, leukodystrophies. We can prove these ARE ischemic microinfarcts with diffusion imaging.”
The Menopause Specialist dropped the bombshell: “There’s a DIRECT CORRELATION between hot flashes and white matter lesions, proven in SWAN’s Ms Brain study. I was horrified to learn this. My entire career, I called these ‘normal for age’ in women’s scans. We tell women not to treat hot flashes unless they’re ‘bothersome enough.’ We’re letting them have tiny strokes!”
The Cardiologist connected the dots: “SWAN showed 60% increased hypertension risk, proportional to hot flash frequency. These are ischemic lesions. Hot flashes → autonomic dysfunction → hypertension → brain ischemia. This is cardiovascular longevity medicine, not just menopause symptoms.”
The Treatment Protocols emerged immediately: Multiple physicians cited plasmalogen deficiency, mitochondrial dysfunction, hormone optimization, VNS therapy, and cardiovascular risk mitigation as intervention pathways.
For longevitydocs: This is longevity medicine in real life: technology and clinical judgment working together.
Multi-specialty collaboration: Neuro, cardio, radiology, hormones, all weighing in.
Biomarkers need context: AI finds patterns, but physicians determine what they actually mean.
Evidence + experience: SWAN data, menopause research, mitochondrial science, and real outcomes.
Mechanisms over symptoms: Autonomic dysfunction, vascular integrity, mitochondrial health.
Precision care: Individualized protocols, not population guidelines.
AI can flag a white-matter lesion. Only a physician knows whether it matters, and what to do next. That’s the clinical layer tech can’t replace.
Not a member yet? Join the debate in the WhatsApp group
Longevity Docs is a highly vetted, invitation-only community for physicians shaping the future of longevity medicine. Apply to connect with our team.

Each week, I highlight studies that could shape the future of longevity medicine. This week is very cardio focused
DNA methylation biomarkers in liquid biopsies

Nature Oncogene review addresses why only a handful of DNA methylation cancer tests have achieved clinical use despite 6,191+ publications. Key findings: (1) Local body fluids (urine, bile, CSF) often outperform blood by 10-80x in sensitivity; (2) Most biomarkers fail due to poor control group selection and lack of clinical utility demonstration; (3) Rigorous validation requires appropriate patient populations, standardized methods, and prospective trials.
For longevitydocs: The same validation standards apply to epigenetic aging biomarkers. As biological age clocks proliferate, knowing what separates validated tests from research tools becomes critical.
Lipoprotein Apheresis in Clinical Practice
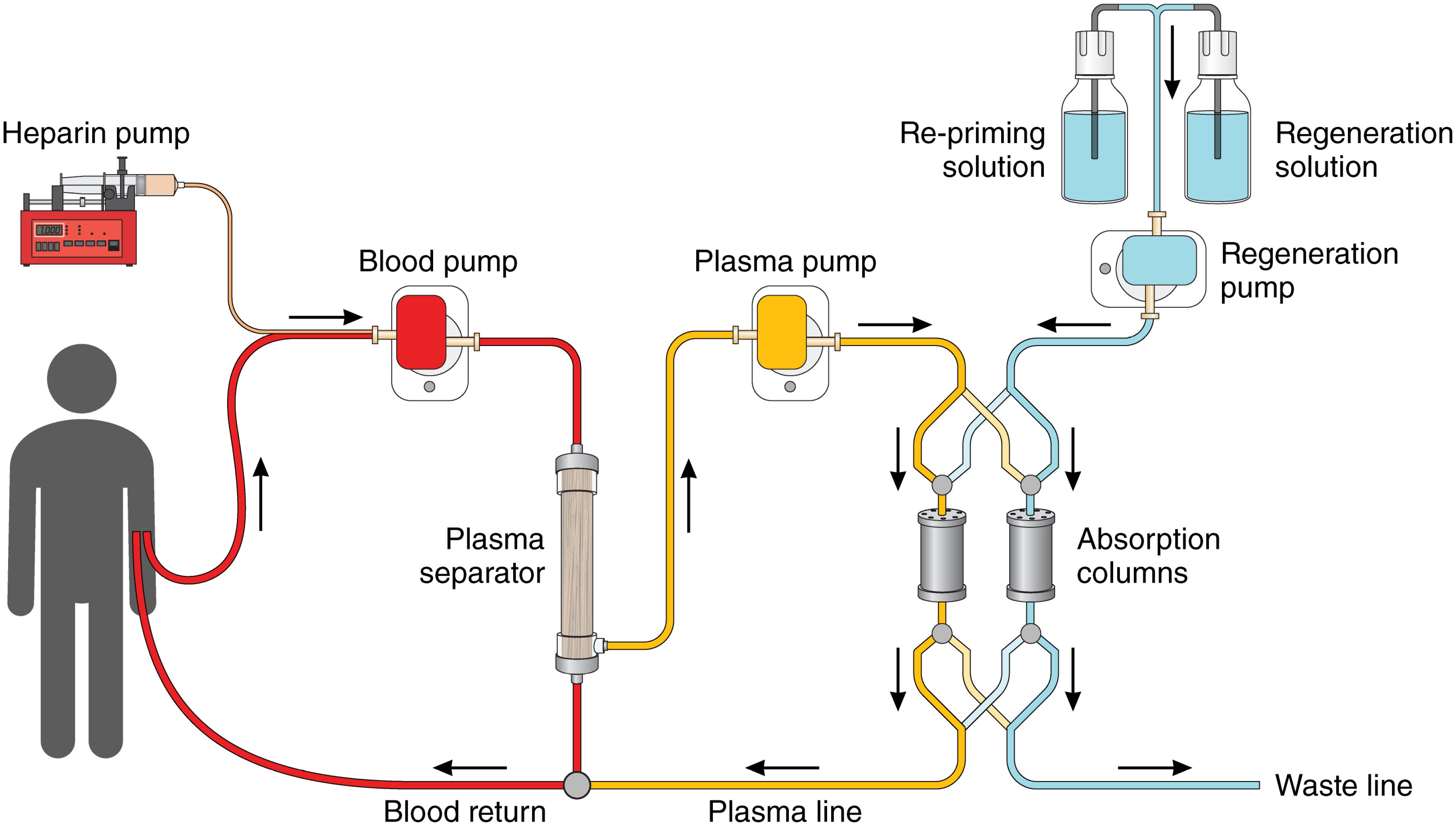
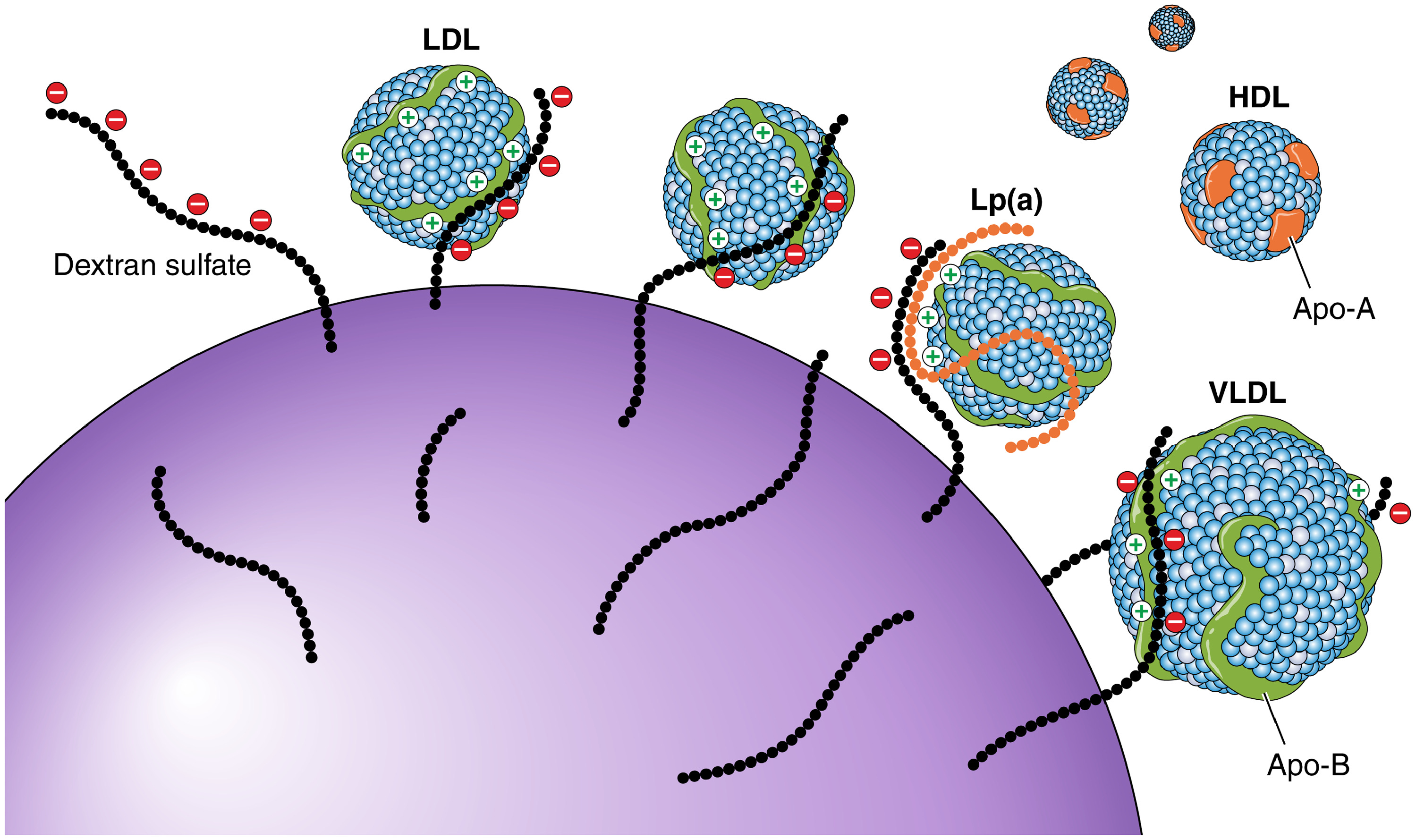
The American Heart Association released a comprehensive scientific statement on lipoprotein apheresis (LA). LA achieves 65-85% acute reduction in both LDL-C and Lp(a) per session, with observational studies showing 63-95% reduction in major adverse cardiovascular events when performed regularly. The procedure is FDA-approved for severe familial hypercholesterolemia patients who fail maximal medical therapy, and also approved under humanitarian exemption for refractory focal segmental glomerulosclerosis. Despite strong evidence for cardiovascular benefit, LA remains drastically underused in the US—only ~400 patients currently receiving treatment versus estimated 11,000-15,000 who qualify. Cost ranges $50,000-$150,000 annually but may be cost-effective given cardiovascular risk reduction comparable to PCSK9 inhibitors at higher baseline risk.
For longevitydocs: When medications fail, lipoprotein apheresis could be the next step. Familiarize yourself with LA criteria and identify regional apheresis centers for complex lipid referrals.

Every week, I track funding, FDA approvals, product launches, and breakthrough announcements shaping longevity medicine.
Function Launches Medical Intelligence Lab to Decode Longevity with AI and 100+ Biomarkers
Function’s Medical Intelligence launches with three core capabilities:
• Private AI Chat that delivers context-aware explanations grounded in each member’s health data.
• Protocols that turn complex biomarker and imaging insights into simple, practical steps members can implement immediately.
• Upload Health Records, a secure vault for medical history: lab reports, imaging, visit notes that feeds into Medical Intelligence for longitudinal interpretation.
For longevitydocs: Function is building the front door. Longevity physicians have the opportunity to be the clinical layer that turns data into outcomes.
Proteomics: Principles and Advances in Bottom-Up Proteomics

In this article, you get a clear overview of bottom-up proteomics: the gold-standard method for breaking proteins into peptides and analyzing them with LC-MS/MS to understand protein identity, quantity, and function. It explains the core workflow (sample prep, digestion, LC, MS/MS), why trypsin-driven peptide generation is essential, how this approach compares to top-down proteomics, and where the field is heading with advances like single-cell analysis and high-throughput quantitative methods.
For longevitydocs: Proteomics is moving from research labs to clinical practice. This will be the next frontier in precision biomarkers after genomics and metabolomics.
New guidance covers AI-based biomarkers for cancer care

ESMO introduces the first real framework to validate AI-based biomarkers in oncology: a space that has been exploding with papers and products but lacking any standards. Their new EBAI guidance outlines the minimum requirements before AI tools can be trusted for diagnosis, prognosis, or treatment decisions. They also released LLM guidance to help clinicians use tools like ChatGPT safely in patient support, education, and clinical documentation.
ESMO classifies AI biomarkers into three groups:
Class A – AI that measures existing biomarkers using the same data (e.g., automated quantification).
Class B – AI that infers known biomarkers indirectly (e.g., screening large populations through histology, then confirming positives with molecular tests).
Class C – New AI-derived biomarkers trained directly on real patient outcomes (prognostic or predictive).
For longevitydocs: AI is powerful, but without validation standards, it shouldn’t guide care. EBAI is meant to set the baseline for regulation, clinical adoption, and industry development.
Introducing Labs by Hims & Hers
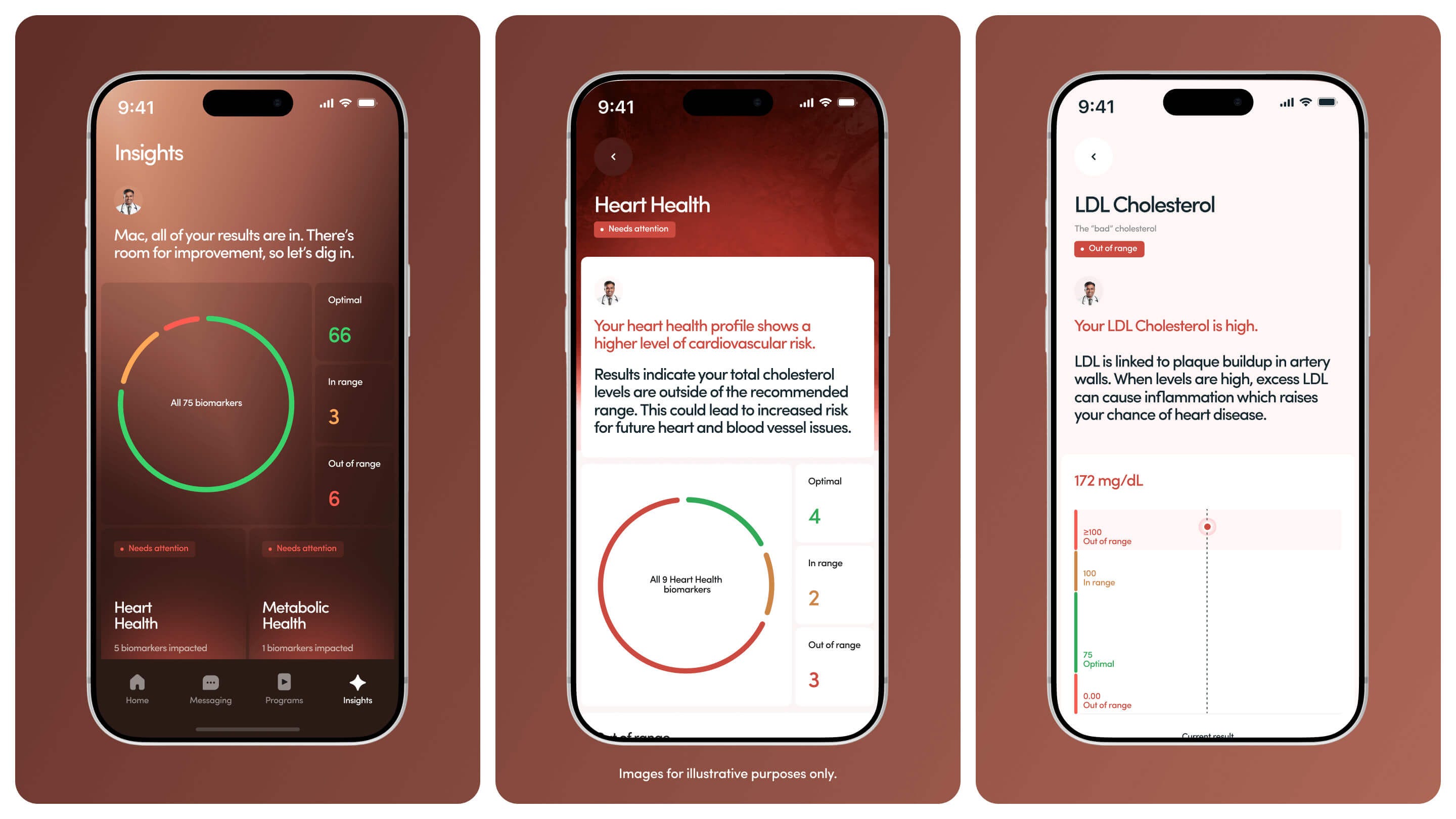
Hims & Hers just launched Labs, a consumer-facing platform offering affordable access to 120 biomarkers across 10 core health domains (heart, metabolism, hormones, inflammation, stress, etc.). Users pick a plan, get a blood draw, and receive results directly in the app, paired with a personalized, doctor-developed action plan that includes lifestyle guidance and optional treatment pathways. The platform tracks progress over time and plans to expand into at-home testing devices, brain and bone biomarkers, and advanced diagnostics at a fraction of traditional costs.
For longevitydocs: mainstream preventive testing is becoming accessible, personalized, and digital, and consumers are being trained to expect it.

AI & TECH MASTERMIND | JANUARY 31, NYC
We’re bringing together 150 longevity physicians building AI-powered longevity practices.
If you’re still figuring out which AI tools are HIPAA-compliant, how to integrate wearables into clinical decisions, or whether proteomics is ready for practice, this is where you get answers from physicians already doing it.
What we’re covering:
Next-gen biomarkers (proteomics, epigenetics, multi-omics)
Wearables and continuous monitoring: clinical-grade vs. wellness theater
NeuroTech and brain aging protocols
Performance metrics that track biological age
AI imaging that catches what radiologists miss
Tech stacks that actually work (EMR integration, dashboards, APIs)
Clinical workflow tools: triage, documentation, protocol generation
AI-powered practice growth without physician burnout
The debate: frontier tech vs. what’s ready now
Your Monday morning action plan: 90-day implementation roadmap
Small group. Curated. Limited to 150 Physicians only.
VIP (50 spots) - Includes private dinner with speakers
In-Person (limited) - Full access to all sessions and networking
Virtual - Live-stream and replay for those who can’t travel
Early-bird ends December 15.
Applications reviewed on a rolling basis. We’re looking for physicians serious about building AI-enabled longevity practices.
Where to Find Us
San Francisco · Dec 5 - Longevitydocs Table
Novato · Dec 6-8 – Longevity Clinic Roundtable
Las Vegas · Dec 12-13 – A4M Conference
Las Vegas · Jan 6-9, 2026 – CES
New York · January 31 – Longevitydocs AI/Tech Mastermind
Cannes, France · June 9-11, 2026 – Longevitydocs Summit

The world’s largest physician network in longevity medicine
longevitydocs.™ is the world’s largest physician network in longevity medicine, serving 600+ vetted physicians across 50+ countries. We unite physicians, industry, and institutions to build the trusted global infrastructure that makes longevity medicine the new standard of care.

Our Pioneering Approach: Uniting Science, Clinical Practice, and Culture
Professional Network
Global Longevity Community: A curated community of leading longevity physicians fostering peer learning, clinical collaboration, and professional growth
Medical Education
Certified longevitydocs.™ (CLD): The first structured, physician-led clinical curriculum for longevity medicine - comprehensive, evidence-based, and practice-ready.
Clinical Research
Longevity Research Network: Clinical research infrastructure enabling rapid generation of real-world evidence across the Longevity Docs network.
Cultural Experiences
Global Events: From Cannes to New York, our Summits, Awards, Masterminds, and Jefferson Dinners convene top researchers, clinicians, investors, and government officials to shape longevity medicine’s growth, investment, and policy.
Intelligence
Strategic Insights: Weekly syntheses of scientific breakthroughs, clinical best practices, business signals, and global market analysis for Fortune 500 companies - the industry’s trusted source of intelligence.
Not a member yet? Longevity Docs is an invitation-only network of 600+ physicians shaping the future of longevity medicine through clinical collaboration, certification, and global events.
Subscribe to the Longevity Docs Newsletter
Stay connected with a global network of 500+ physicians in 50+ countries advancing longevity medicine. Get evidence-based insights, clinical updates, and exclusive access to the community shaping the future of longevity care.
Newsletter Disclaimer: