

Social Longevity Is the New Superpower
#92 Weekly Longevity Medicine Intelligence

Hey Doc,
4:45am. Like every Sunday, blank page. What’s this week’s cover story?
Then I remembered yesterday. Press day. A reporter asked me for my most underrated longevity secret. When I said community, she looked surprised. Then very interested.
Social longevity is the bet every patient, every doctor, every society should be making. In an era of AI and self-optimization, the highest-leverage move is the oldest one: community, purpose, altruism.
Took a break for lunch in sunny SoHo with family and friends. Walking the talk.
Back at the desk, inspired by the street art on the way home, designing the cover.
4:57pm. App is live. Cannes is five weeks out. Newsletter 92 is out.
Dr. David Luu, Founder, longevitydocs.™

Every Wednesday, we ship something new for this community. Features, experiences, and products built by physicians, for physicians. The platform grows because you do.
APP
The Longevitydocs mobile app is live.
Longevity medicine in one place. In your pocket. Every day.
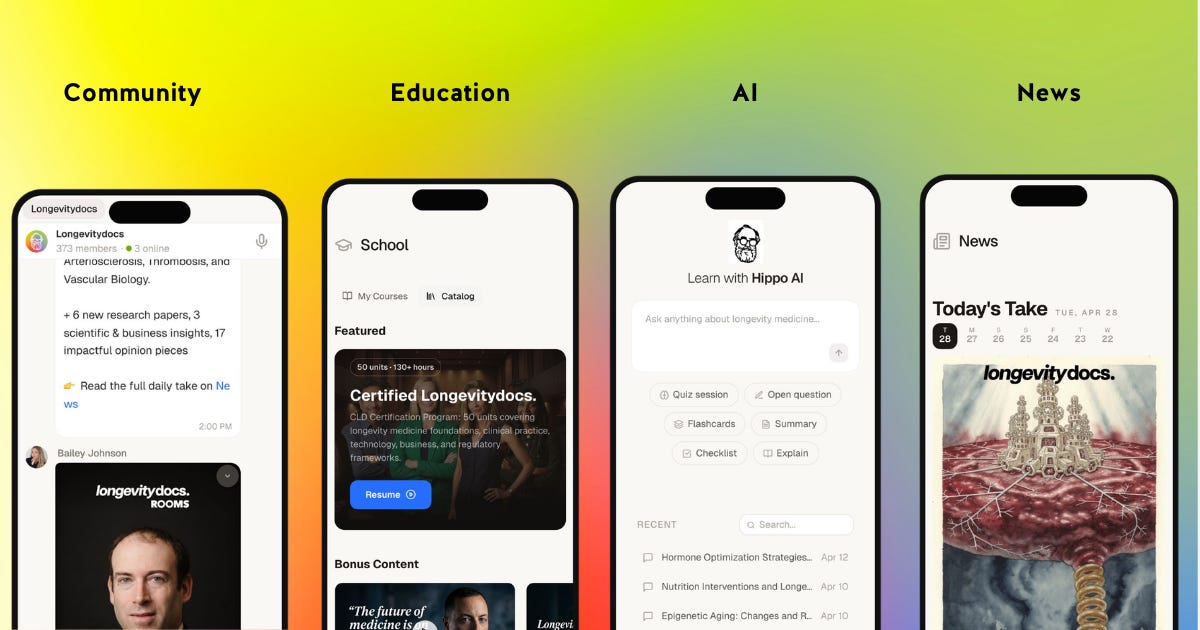
Here’s what’s inside:
News. Curated longevity medicine intelligence, daily. New research, business moves, regulatory shifts. Two minutes. You’re current.
Hippo AI. Trained on the full CLD curriculum. Ask it anything. Generate quizzes. Build flashcards. Get protocol summaries before a patient visit. Your second brain for longevity medicine.
School. The complete Certified Longevitydocs program. 50 units. 100+ hours. Syncs between desktop and mobile so you can learn in fifteen-minute windows between patients.
Community. Meet physicians, exchange protocols, debate the literature, share clinical insights in real time. Plus live Rooms with guest experts every week.
Every doctor should be a longevity doctor. Now you can carry that mission in your pocket
If you’re a member, download and log in with your existing credentials. If you’re not yet a member: apply to join here
Available now on the Apple App Store. iPhone only. Android coming soon.
ROOM OF THE WEEK
How Should We Treat High Lp(a)?
5 Key Takeaways from LongevityDocs Rooms
by Dr. Giovanni Campanile
1. Test once, then test the family. Lp(a) is 80-95% genetic. A first-degree relative has a 50% chance of also being elevated. One test per patient, one conversation per family. Flag >30 mg/dL even though guidelines say >50.
2. You cannot lower Lp(a) directly, so lower everything else harder. PCSK9 inhibitors are the go-to today. Push ApoB to <40 (not the usual <60). Keep statins despite the paradoxical 10-20% Lp(a) rise. Add aspirin for the thrombogenic profile. Add HIIT for the plaque reduction data.
3. Image the coronaries before starting HRT in postmenopausal women with high Lp(a). If plaque looks unstable, stabilize first. Transdermal over oral in year one. Women who started HRT premenopausally and enter menopause on it do not carry the same plaque-rupture spike risk.
4. Three RNA therapies landing in 2026-2027 will change the field. Pelacarsen (Lp(a) down >80%), olpasiran (down 95%, quarterly injection), muvalaplin (oral). One of them may become the first medical therapy for aortic stenosis.
5. Obicetrapib is the sleeper for the trifecta patient. Oral CETP inhibitor, EU-approved, lowers LDL 50% plus Lp(a) meaningfully, and slows Alzheimer’s progression in ApoE4 carriers. If your patient has elevated ApoB, Lp(a), and ApoE4, this is the one to watch.
Join our next Room tomorrow

Rooms are available on the longevitydocs.ai

Each week, I try to explore one idea that could advance longevity medicine and hopefully support physicians in bringing it to life.
Social Longevity: 12 Reasons Community Is the Longevity Superpower
Did we make longevity selfish? Most protocols and innovations in this space are self-centered, performative, and isolating. The entire movement has been reduced to a single-player game.
But being social is not a lifestyle trend. It is the oldest survival mechanism our species has. What I call social longevity is the combination of community, purpose, and altruism. For 300,000 years, humans survived because we belonged. That is what separated us from other species. Not our teeth, not our speed. Our ability to cooperate, bond, and build trust across generations.
Isolation kills. Comparable to smoking 15 cigarettes a day. The WHO linked social disconnection to 871,000 deaths annually. Most longevity clinics do not screen for it.
The most powerful longevity intervention is not a molecule. It is other people. It is free. Yet it is the greatest investment you will ever make in your health.
Here are twelve reasons why.
1. Inflammation. Loneliness elevates CRP, IL-6, and fibrinogen in a dose-dependent manner. The more isolated you are, the more inflamed you become. Social connection suppresses NF-kB inflammatory signaling at the genomic level. Belonging could be anti-inflammatory.
2. Immunity. Isolated individuals show reactivation of latent herpes viruses. Wound healing slows by 40 percent. NK cell activity declines. Connection keeps your immune system vigilant.
3. Stress Hormones. Loneliness compresses cortisol dynamic range, reducing your ability to mount and recover from stress. Chronic isolation produces cortisol blunting, the same pattern seen in PTSD and burnout. Social interaction restores HPA axis flexibility.
4. Cardiovascular. Loneliness increases heart disease risk by 45 percent and stroke by 28 percent. Social integration reduces cardiovascular mortality by two to three times independent of traditional risk factors.
5. Telomeres. Social isolation is associated with shorter telomere length. Caregiving stress without social support accelerates telomere shortening by ten years of cellular aging. Disconnection ages you at the chromosomal level.
6. Cognition. Social isolation has a direct causal effect on cognitive decline. Loneliness increases dementia risk by 40 percent. Purpose reduces Alzheimer’s risk by 2.4 times, even with amyloid pathology at autopsy.
7. Behaviors. Social isolation activates the Conserved Transcriptional Response to Adversity: 53 pro-inflammatory genes upregulate, antiviral defenses shut down. Purpose-driven well-being reverses this pattern. Pleasure-driven well-being does not. Your genome distinguishes between types of happiness.
8. Nervous System. Social engagement activates the ventral vagal complex, promoting parasympathetic dominance. This could predict greater cognitive flexibility and lower inflammatory gene expression. Connection calms your sympathetic nervous system at a level you cannot consciously control.
9. Oxytocin. Social bonding triggers oxytocin release, which modulates the HPA axis, has anti-inflammatory properties, and increases trauma resilience. Prosocial behavior activates dopaminergic reward circuits. Helping others feels good because, biologically, it is good.
10. Purpose. Purpose reduces all-cause mortality by 15 percent across 136,000+ participants. Ikigai is associated with a 36 percent reduction in cardiovascular mortality over seven years.
11. Generosity. Volunteering cuts mortality risk by 22 to 44 percent. Giving support is more protective than receiving it. Prosocial spending lowers cortisol more than self-directed spending across cultures.
12. Network Effect. Health behaviors propagate through social ties up to three degrees of separation. Your friends’ friends’ friends are shaping your physiology. Isolation is not just the absence of connection. It is the absence of the upward pull that connected people exert on each other.
What’s Next
Who do you eat dinner with? Who calls you when something goes wrong? What are you building that is bigger than yourself? Most longevity intakes never ask these questions. They should.
My next passion project: building a Social Longevity Score. Three pillars. Connection. Purpose. Altruism. Measured with the same rigor we apply to biomarkers, correlated with the same panels we already run, and scored in a way a clinician can act on. In the coming months I will go deeper on each of these twelve reasons, and the research behind it.
Every doctor should be a longevity doctor. But no longevity doctor should practice alone.
A Note on the Evidence
These are associations and mechanisms, not clinical trials. The data suggests social connection is biologically active. It does not yet prove that prescribing community saves lives the way prescribing a statin does. We need evidence-based research using multi-omics (genomics, proteomics, metabolomics, epigenomics) integrated with longitudinal outcomes to move from association to intervention. If social disconnection carries the mortality risk of 15 cigarettes a day, we owe it that rigor. The tools will never be ready if nobody builds them.
Holt-Lunstad J, Smith TB, Layton JB. Social relationships and mortality risk: a meta-analytic review. PLoS Medicine. 2010;7(7):e1000316.
U.S. Surgeon General. Our Epidemic of Loneliness and Isolation. Washington, DC: HHS; 2023.
WHO Commission on Social Connection. Social connection linked to improved health and reduced risk of early death. June 2025.
Smith KJ, et al. The association between loneliness, social isolation and inflammation: a systematic review and meta-analysis. Psychosomatic Medicine. 2020;82(8):801-812.
Cole SW, et al. Social regulation of gene expression in human leukocytes. Genome Biology. 2007;8(9):R189.
Cole SW. Human social genomics. PLoS Genetics. 2014;10(8):e1004601.
Fredrickson BL, et al. A functional genomic perspective on human well-being. PNAS. 2013;110(33):13684-13689.
Van Bogart K, et al. Daily loneliness and cortisol dynamic range. Biological Psychology. 2026;109247.
Stout DM, et al. Loneliness and blunted cortisol reactivity to social exclusion. Social Neuroscience. 2023;18(4):289-301.
Haucke M, et al. Loneliness and cortisol during COVID-19 lockdown. Psychoneuroendocrinology. 2022;144:105894.
Valtorta NK, et al. Loneliness and social isolation as risk factors for coronary heart disease and stroke. Heart. 2016;102(13):1009-1016.
Berkman LF, Syme SL. Social networks, host resistance, and mortality: a nine-year follow-up study of Alameda County residents. American Journal of Epidemiology. 1979;109(2):186-204.
Glaser R, et al. Stress-related impairments in cellular immunity. Psychiatry Research. 1985;16(3):233-239.
Kiecolt-Glaser JK, et al. Slowing of wound healing by psychological stress. The Lancet. 1995;346(8984):1194-1196.
Pressman SD, et al. Loneliness, social network size, and immune response to influenza vaccination. Health Psychology. 2005;24(3):297-306.
Steptoe A, et al. Loneliness and neuroendocrine, cardiovascular, and inflammatory stress responses. Psychoneuroendocrinology. 2004;29(5):593-611.
Epel ES, et al. Accelerated telomere shortening in response to life stress. PNAS. 2004;101(49):17312-17315.
Kivimaki M, et al. Social disadvantage accelerates aging. Nature Medicine. 2025;31:1635-1643.
Hale JM, et al. Causal effect of social isolation on cognitive function. Journal of Gerontology B. 2026;gbaf254.
Sutin AR, et al. Loneliness and risk of dementia. Journal of Gerontology B. 2020;75(7):1414-1422.
Boyle PA, et al. Effect of a purpose in life on risk of incident Alzheimer disease. Archives of General Psychiatry. 2010;67(3):304-310.
Porges SW. The polyvagal perspective. Biological Psychology. 2007;74(2):116-143.
Colzato LS, et al. Variable heart rate and a flexible mind. Cognitive, Affective, and Behavioral Neuroscience. 2018;18:600-610.
Gimpl G, Fahrenholz F. The oxytocin receptor system. Physiological Reviews. 2001;81(2):629-683.
Sharma SR, et al. Oxytocin and trauma resilience. Pharmacology and Therapeutics. 2020;214:107602.
Moll J, et al. Human fronto-mesolimbic networks guide decisions about charitable donation. PNAS. 2006;103(42):15623-15628.
Cohen R, et al. Purpose in life and its relationship to all-cause mortality and cardiovascular events: a meta-analysis. Psychosomatic Medicine. 2016;78(2):122-133.
Sone T, et al. Sense of life worth living (ikigai) and mortality in Japan: Ohsaki Study. Psychosomatic Medicine. 2008;70(6):709-715.
Okun MA, et al. Volunteering by older adults and risk of mortality: a meta-analysis. Psychology and Aging. 2013;28(2):564-577.
Brown SL, et al. Providing social support may be more beneficial than receiving it. Psychological Science. 2003;14(4):320-327.
Dunn EW, et al. Spending money on others promotes happiness. Science. 2008;319(5870):1687-1688.
Christakis NA, Fowler JH. The spread of obesity in a large social network over 32 years. New England Journal of Medicine. 2007;357(4):370-379.
Christakis NA, Fowler JH. The collective dynamics of smoking in a large social network. New England Journal of Medicine. 2008;358(21):2249-2258.
Cacioppo JT, Fowler JH, Christakis NA. Alone in the crowd: the structure and spread of loneliness in a large social network. Journal of Personality and Social Psychology. 2009;97(6):977-991.

Every week, the Longevity Docs Chat feels like a front-row seat to the future of medicine. Here’s what had doctors buzzing:
HRV: Are Doctors Built Different?
It started with a simple question about magnesium glycinate and a spike in HRV on WHOOP. One member quickly flagged the confounders:
WHOOP’s HRV isn’t an overnight average, it’s weighted towards deep sleep. And detecting deep sleep itself uses HRV, creating a circular measurement problem.
Another physician agreed and raised excipient sensitivity in specific supplement formulations as a variable worth checking.
Then a member shared something remarkable: 840 days of simultaneous WHOOP and Oura data showing chronically low HRV that never once reached normal range. But within that low range, HRV still predicted recovery with strong correlation (r = 0.68, 834 nights).
Best-HRV nights: recovery 79%. Worst: 47%. System is adaptive. Just running on a different scale.
That prompted a provocative hypothesis from another physician:
doctors may carry a constitutional low-HRV phenotype.
The idea is that elite test-takers are selected in part for higher baseline sympathetic tone, a trait that helped survive the MCAT but may leave us running hot for life. He cited research from the Israeli Defense Forces showing autonomic regulation as an independent predictor in elite military selection.
A colleague pushed back thoughtfully:
I’d be cautious about extending this to a constitutional low-HRV phenotype or selection bias in physicians. The evidence I’m aware of tends to support state over trait, with training and practice environments shaping autonomic patterns over time.
Key Takeaway:
Stop comparing your HRV to population norms. Within-individual trends matter more than absolute values. Track your own baseline. Measure your own trajectory. And if your HRV runs low, consider the possibility that it reflects your autonomic wiring, not just your lifestyle. The data to prove or disprove that is not here yet. But the question is worth asking.
Elevated Ferritin: Case Study
Community Case: Elevated Ferritin with Normal Iron Studies
A member posted a clinical question:
ferritin at 482, positive for one HFE H63D variant, normal iron and TIBC. What else beyond phlebotomy?
What followed was a 24-hour clinical deep dive involving gastroenterologists, cardiologists, and longevity physicians across multiple time zones.
One physician laid out the systematic workup:
Check transferrin, TIBC, liver enzymes, CRP, ESR, uric acid, LDH. Rule out alcohol, intense exercise within 72 hours, and inflammation.
A cardiologist cut to the core:
Measure transferrin saturation first. If TSAT is above 45%, this is iron overload. A common cause of elevated ferritin is fatty liver or a neoplasm or any other inflammatory condition.
Another member added hepatitis screen, CGM, and liver imaging to the list, then shared a case where unexplained hyperferritinemia turned out to be SAPHO syndrome presenting as severe acne and dermatitis.
Two other physicians shared their own cases of persistent ferritin elevation post-COVID (ranges of 377 to 700) with normal inflammatory markers and no clear etiology. One is trialing lactoferrin with an 8-week follow-up.
One member challenged the group to think upstream: why is the body sequestering iron before we rush to treat? She cited evidence on iron withholding as an immune defense mechanism.
Another connected it to hepcidin upregulation in patients on rapamycin, linking mTOR inhibition to mild iron deficiency anemia.
Key Takeaways
Isolated ferritin elevation is never simple. TSAT is your first branch point. Then think broader: liver, inflammation, autoimmune, post-COVID, and medication-induced causes including rapamycin. Do not reflexively phlebotomize without understanding the mechanism.

AI vs. ER Physicians in Triage Differential Diagnosis
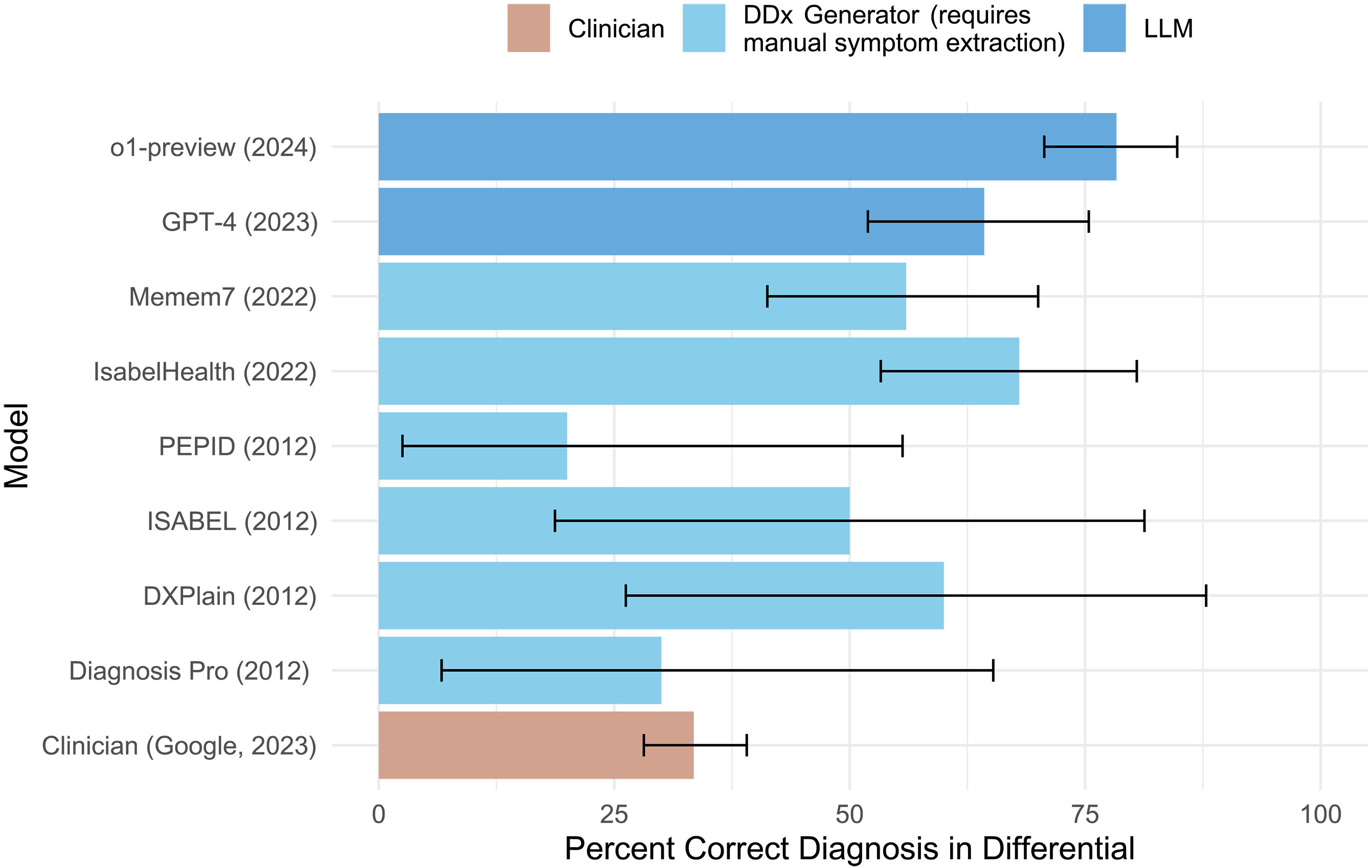
Study published in Science showing AI models outperforming real ER physicians in triage differential diagnosis across multiple phases of clinical reasoning. Why it matters: Models used were from mid-2025. Current frontier models are significantly stronger. The gap between AI and physician performance at pattern recognition is widening. The physician value shifts to context, continuity, and care. Science
Caloric Restriction Reduces Inflammaging Through Complement C3a Suppression
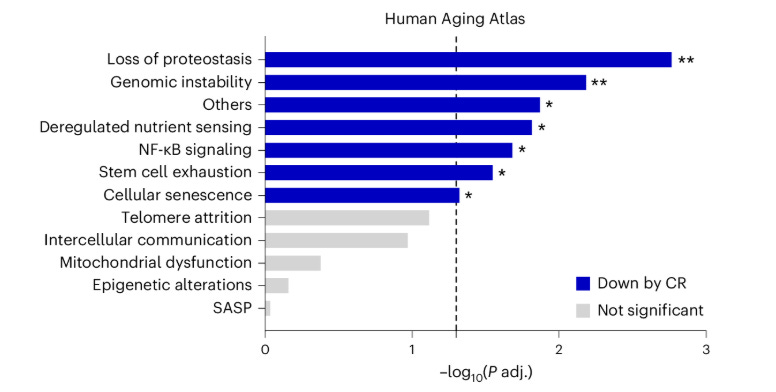
Yale researchers analyzed proteomics from the CALERIE trial and identified complement C3a suppression as the key mechanism behind caloric restriction’s anti-aging benefits. The source: a macrophage subset in visceral adipose tissue that expands with age and drives complement activation. Neutralizing C3a in aged mice reduced inflammation and shifted macrophages toward an anti-inflammatory profile. An FDA-approved C3 inhibitor (pegcetacoplan) already targets this pathway.
Why it matters: C3a is now a measurable biomarker for inflammaging, visceral fat is confirmed as the epicenter, and a druggable CR-mimetic pathway already has an approved drug.
Current Status and Future Perspectives on Long COVID Pathophysiology
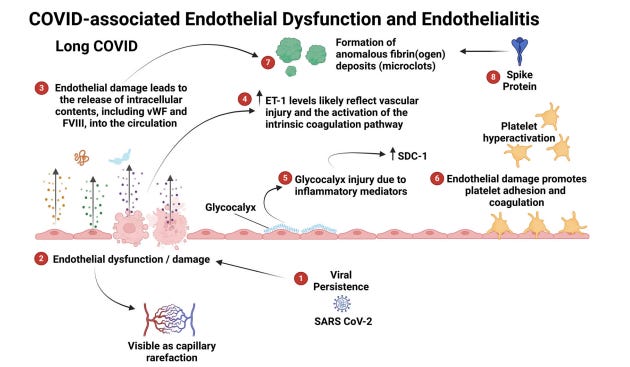
Review of 400+ million cases globally. Five mechanisms identified: immune dysregulation, viral persistence, microclotting, autonomic dysfunction, and neuroinflammation. Spike protein detectable in 60% of patients at one year. No validated biomarker. No cure. Why it matters: These are the same mechanisms we target in aging. Long COVID is accelerated biological aging triggered by infection. Our frameworks apply directly. Communications Medicine

They Are Certified Longevity Docs (CLD)
Congratulations to the physicians who earned their Certified Longevity Docs (CLD) designation this month. Empowering the next generation of physicians committed to the standard of evidence-based longevity medicine education.
Dr. Jorge Perez grew up in Cuba near a medical center, which inspired his desire to work in healthcare. Now a Cardiologist at the Chen Senior Medical Center in Miami, Dr. Perez focuses on supporting his senior patients in building happy, healthy lives. His recent research includes Echocardiographic Features of Longevity in Centenarians, noting that centenarians represent an under-studied population within cardiovascular medicine. He received Fellow of the Year Award for Excellence in Professionalism and Compassionate Care at Mount Sinai Medical Center of Florida.
Dr. Anna Chromcova is the Co-Founder and Medical Director of Doktůrek.ai, on a mission to revolutionize primary care. She is a graduate of First Faculty of Medicine, Charles University in Prague, starting her career in medicine as a Radiologist. Her passion for technology led her to join Carebot at Medical Director, a medical software company using AI and Machine Learning to evaluate radiology imaging. In addition to building Doktůrek.ai, she is a general practitioner in the Czech Republic where she supports her patients with hyper-individualized care throughout the their health journey.
The Certified Longevity Doctor designation is the standard our community is building. If you practice longevity medicine with evidence and accountability, this is the credential that says it.

Every week, I track funding, FDA approvals, product launches, and breakthrough announcements shaping longevity medicine.
CARE
CVS launches AI health platform with Google
CVS Health partnered with Google Cloud to launch Health100, an AI-powered health technology subsidiary. The platform uses Gemini models to deliver cross-network care management across pharmacy, provider, insurer, and PBM channels, with wearable integration and real-time biomarker tracking planned for 2026.
Why it matters: A $102.5B company building AI-driven preventive health infrastructure is moving into the data-rich space longevity medicine pioneered. Physicians who position themselves within these ecosystems early will have an advantage. Those who do not may find retail healthcare defining the category for them.
AI
Google DeepMind Launches AI Co-Clinician

Google DeepMind announced a “triadic care” model: AI agents that interact directly with patients under physician supervision. In blind evaluations, the system recorded zero critical errors in 97 of 98 primary care queries and matched or exceeded physicians in 68 of 140 consultation skills, including guiding physical exams via live video. Experienced physicians still outperformed on red-flag recognition.
Why it matters: AI is moving from information tool to clinical teammate. The physician value is no longer diagnosis. It is judgment, relationships, and the ability to design longitudinal protocols no AI can yet own. Build your practice around what AI cannot replace.
INVESTMENTS
Infinite Epigenetics Acquires Tally Health

TruDiagnostic’s parent company acquired David Sinclair’s Tally Health, creating a vertically integrated platform combining CLIA-certified lab infrastructure, 115+ research partnerships, the world’s largest private DNA methylation datasets, and consumer-facing at-home epigenetic age testing.
Why it matters: Epigenetic testing is moving from research curiosity to scalable infrastructure. The consolidation of methylation data at this scale will accelerate validation of biological age markers we already use. Physicians who can interpret epigenetic data will be essential partners in this ecosystem. Those who cannot will watch platforms deliver longevity medicine without them.
SquareMind Raises $18M for Robotic Skin Imaging

SquareMind’s Swan robot performs automated full-body dermoscopic imaging in minutes. Contactless, AI-paired, designed to track new or changing lesions over time. Round led by Intuitive Surgical founder Fred Moll’s fund. Commercial launch imminent in US and Europe.
Why it matters: 80% of melanomas are new lesions, not existing moles that changed. That makes comprehensive skin mapping a longevity screening imperative. For physicians building skin into their diagnostic framework, this turns a subjective visual exam into structured, trackable data at scale.
POLICIES
FDA Moves to Limit Compounded GLP-1s

The FDA proposed excluding semaglutide and tirzepatide from the 503B bulks list, finding no clinical need for outsourcing facilities to compound these drugs from bulk substances. Public comment open until June 29. Individual patient compounding under physician prescription (503A) remains intact for now.
Why it matters: The regulatory direction is clear. Build protocols around branded or FDA-approved pathways and document clinical rationale carefully. Affordable access through compounding is narrowing, not expanding. Be aware for your patients
PHARMA
LSD-Based Anxiety Drug Nears FDA Approval

Definium Therapeutics expects Phase 3 results for DT120, an LSD-based treatment for generalized anxiety disorder. Phase 2 showed 78% clinical response and 50% remission after four weeks. No new anxiety drug has been approved since Cymbalta in 2007. All 7,000 existing Spravato centers could deliver it.
Why it matters: DT120 works through 5-HT2A receptor activation and neuroplasticity, not symptom suppression. If approved, the first new class of anxiety treatment in nearly two decades. Mental health is a longevity intervention. This is the mechanism catching up to that reality.
CULTURE
Longevity Travel Goes Mainstream

ELLE reports luxury hospitality is embedding real diagnostics into the guest experience. Santa Monica Proper Hotel offers 160+ biomarker panels on-site. Clinique La Prairie leads clinical wellness tourism, now valued at $18B and projected to reach $48.2B by 2033. Properties are integrating pharmacogenetic testing, red light therapy, and IV drips alongside indigenous healing traditions.
Why it matters: Hotels are building longevity medicine into hospitality at scale. New referral channels, consulting opportunities, and clinical partnerships outside the clinic. People want longevity medicine woven into daily life, not confined to a waiting room.
Qantas Redesigns Long-Haul Flights Around Longevity

Qantas is adding wellbeing zones on its new A350 fleet for Sydney to London and Sydney to New York routes, launching 2027. Stretching handrails, exercise programs, hydration therapy. Clinical research with the University of Sydney confirmed the need to move during flights is physiological, not a luxury.
Why it matters: An airline just cited clinical research to redesign the flight experience around movement, hydration, and circadian reset. Longevity thinking at 40,000 feet. For physicians flying to Cannes in June: the flight is part of the protocol.

The Cannes Ecosystem Map
Cannes. June 9–11, 2026. Palais des Festivals.
We built this summit on a simple belief: longevity medicine will not scale inside silos. It scales when the hospital system, the AI lab, the beauty conglomerate, the clinic, the investor, and the regulator are in the same conversation. That conversation happens here.
This is the operating table where the ecosystem gets built.
Who you’ll meet in Cannes:
Health Systems: Mayo Clinic. Mount Sinai. Sheba Medical Center. Cedars-Sinai.
Academic Societies: American College of Cardiology, The Academy of Geroscience
Clinics: Atria Institute, Clarify Clinic, Fountain Life, Next Health, Extension Health, Neko Health
Big Tech & Consumer Health: Samsung, Noom, Hims & Hers, Hone Health, OpenLoop, Eli Health
Beauty & Longevity: Lancôme, L’Oréal Group
Investors & Capital: TPG, Primetime Partners
Public Sector: City of Cannes, U.S. federal longevity initiatives.
The agenda includes: Nir Barzilai on the state of geroscience. Ami Bhatt and Zahi Fayad on the AI-augmented physician. Vania Lacascade on Lancôme’s longevity launch. Hon Pak on Samsung’s ambient longevity ecosystem. Saeju Jeong on scaling longevity to millions. Mayo, Mount Sinai, and Sheba on the longevity hospital of the future. Women’s Longevity 360. The Longevity Clinic Standard. The economics of a profitable clinic.
Off stage: White Party on Majestic Beach. Sunrise Run Club on La Croisette. Bioharmony on the beach. Leadership lunches on the sand. Black-tie Gala and the inaugural Certified Longevitydocs™ graduation at the Carlton.
Every seat in this room was earned. Every name on this list is building something. The question is not whether longevity medicine becomes the standard of care. It is who builds the infrastructure that makes it possible.
Will you be in the room?

Mastermind Replays Now Available

3 Masterminds. 3 topics reshaping longevity practice: AI & Tech, Peptides, and Hormones - featuring the dozens of faculty. Trusted by hundreds of physicians
Conferences
Jun 9–11 — Longevity Docs Cannes: Awards & Summit
Jun 29–Jul 1 — A4LI H-SPAN Summit · Washington, DC Longevity medicine meets regulation and policy.
Aug 24–28 — ARDD · Boston Where aging research meets drug discovery.
Oct 17 — Longevity Docs Skin Longevity Mastermind · New York, NY.

The Home of Longevity Medicine
longevitydocs.™ is the world’s leading longevity physician community - 1,000+ physicians across 68 countries united by a single conviction: every doctor should be a longevity doctor. Founded by Dr. David Luu, the platform offers its members network, education, and experience with the mission to democratize longevity medicine.
Not a member yet? Join longevitydocs™
We’re a physician-only network. Curated. Vetted. Built on trust. If you’re committed to practicing longevity medicine with rigor, peer support, and shared standards → this is your community. Apply to connect with our team.
Longevity medicine is the personalized, evidence-based practice of modifying the root mechanisms of aging (biological, cognitive, and psychosocial) before they become disease, extending healthspan, not just lifespan. Using advanced diagnostics, precision interventions, and AI-enabled monitoring, it translates measurement into action across every medical discipline. Success is measured in functional capacity, vitality, and disease-free years.

Subscribe to the Longevity Docs Newsletter
Longevity medicine is moving fast. Every week, we bring you what matters: clinical insights, research signals, and perspectives from 1,000+ physicians across 68 countries. One newsletter. Built for the physicians shaping this field.
Editorial Disclaimer: