

Should Doctors Build a Personal Brand?
#88 Weekly Longevity Medicine Intelligence


Hey Doc,
It is 5pm. I just finished our annual lunch, surrounded by 30 people. Family. Friends. Every guest can bring a friend. No guestlist.
We cooked. We made fun of each others. We danced. Someone played guitar. Someone pulled out the dominoes.
One tradition I have kept. Before we eat, everyone stands and shares one word of gratitude. That is it. No speech. No performance. Just presence before the meal.
What struck me today was not the food or the music. It was the room. People who had never met, laughing like they had known each other for years.
This is my longevity way. A Sunday lunch that runs three hours longer than planned. Gratitude shared before the first bite. A community that feeds you before the food even arrives.
We talk a lot about health optimization. Today I wanna talk about life optimization.
Dr. David Luu - Founder, longevitydocs.™

Each week, I try to explore one idea that could advance longevity medicine and hopefully support physicians in bringing it to life.
Should Doctors Build a Personal Brand? 5 Pros and 5 Cons.
This cover story started in our chat. One doctor shared the social media agency he uses. Full production. Other docs chimed in. Some impressed. Some skeptical. Most asking the same thing quietly: should I be doing this too?
It made me think.
Doctors have always been a brand.
This is not new. This is ancient.
Hippocrates understood it. The physician’s reputation was sacred. How you showed up at the bedside. How you delivered a diagnosis. Whether you listened before you spoke. That was your brand before the word existed.
For centuries, doctors were recognized by five things: knowledge, expertise, service, bedside manner, and outcomes. Your patients knew it. Your community knew it. Referrals came by word of mouth. A doctor’s name carried weight in the village, the town, the hospital corridor.
No one called it branding. But that is exactly what it was.
The AMA banned physician advertising until 1980. But it did not matter. Reputations still traveled. Patients still chose their doctor based on what their neighbor said. Surgeons were still known for steady hands. Family physicians were still known for midnight house calls.
The brand existed. It just lived in conversations, not on screens.
How the brand metrics changed.
Not long ago, the markers of a great physician were clear. He trained at Harvard. She was featured in the New York Times. He published 100 scientific papers. That was the currency. Institutional pedigree. Media validation. Academic output.
Those things still matter. But they are no longer enough.
Today the metrics look completely different. Millions of followers. Celebrity patients. Brand partnerships. A lifestyle that signals success. Entrepreneurial ventures outside the clinic. Political positions. Cultural opinions. A personal story that people follow like a narrative.
The journey itself has become part of the brand.
A doctor used to be judged by where he trained and what he published. Now he is also judged by how he shows up online, what he believes publicly, and whether his story resonates. The CV still opens doors. But the personal narrative is what fills the room.
I am not saying this is better or worse. I am saying it is real. And ignoring it does not make it go away.
What changed.
The principle never changed. Where it lives did.
Google arrived. Suddenly your patients looked you up before they walked in. Your online presence became your first impression.
Social media followed. Doctors could speak directly to patients, to peers, to the public. Some embraced it. Most resisted.
Telemedicine removed geography. A doctor in Miami could treat a patient in Montana. But only if that patient could find them.
Now AI. Patients ask ChatGPT before they ask their doctor. The physicians whose thinking lives online are the ones AI surfaces. The invisible doctor becomes truly invisible.
Each wave raised the stakes. Each wave rewarded the same thing: the doctor who showed up with clarity about who they are and what they stand for.
What does building a brand actually mean?
Not a logo. Not a follower count. Not a production budget.
Your brand is your reputation. It is how people describe you when you are not in the room. It is the principles you defend. The positions you take. The way your patients feel after they leave your office and then search your name.
You already have one. The only question is whether you are shaping it or leaving it to chance.
5 Pros: Five reasons a brand can build you.
1. Trust. Medicine has always run on trust. But trust used to travel slowly: word of mouth, hospital corridors, a neighbor's recommendation. Now it travels at the speed of a Google search. Your brand is how trust scales. It communicates your principles before you speak. Your values before a patient books. Your personality before they walk through the door. The physicians patients stay with longest are not always the most credentialed. They are the most known, the most consistent, and the most believed.
2. Expertise. You can be the best longevity physician in your city and be completely unknown outside your zip code. A brand changes that. Every article you publish, every talk you give, every position you take publicly extends your clinical thinking beyond the exam room. Expertise without visibility is a ceiling. Your brand removes it. The physicians shaping this field are not necessarily smarter than you. They are just more visible.
3. Discovery. Your patients are searching right now. Not for a doctor. For an answer. For someone who understands what they are going through. If your name does not come up, someone less qualified fills that space. That is not a marketing problem. That is a patient care problem. A brand makes you findable by the right patients, at the right moment, before they ever pick up the phone.
4. Autonomy. The physicians with the most freedom are not the ones with the most credentials. They are the ones known for something. A strong brand gives you leverage over your schedule, your pricing, your patient selection, and your career trajectory. It is the difference between building a practice around your life and building a life around your practice. Brand is not vanity. It is the infrastructure of autonomy.
5. Opportunity. A brand compounds. Every talk builds on the last. Every published piece adds to the body of work. Every consistent post expands the network. Three years of clarity and consistency will transform your reach, your reputation, and the opportunities that find you: advisory boards, partnerships, media, speaking, investment. The physicians who built their brand five years ago are not working harder than you. They are just receiving more inbound than you. That gap closes the day you start.
5 Cons: Five Ways a Brand Can Break You.
1. Time. Building a brand is not a weekend project. It is a long game that demands consistent attention (content, presence, engagement, strategy) on top of a clinical schedule that already has no slack in it. The physicians who burn out on brand building are not the ones who tried too hard. They are the ones who underestimated the commitment before they started. A neglected brand does more damage than no brand at all.
2. Dilution. Slowly. That is how it happens. One compromised post. One paid ad. One position taken for reach instead of truth. You became a physician because you believed in something. The moment your brand starts chasing engagement instead of conviction, you begin trading your purpose for an audience. Your brand should amplify what you stand for. The moment it starts replacing it, stop.
3. Exposure. Everything you say publicly can be taken out of context, challenged, or weaponized. Trolls. Misinterpretation. Regulatory scrutiny. Licensing board complaints. These are not hypothetical. They are the reality of practicing medicine in public. Visibility is power. It is also exposure. Build your brand knowing both are true.
4. Investment. Branding building can costs up to tens of thousand dollar a month. That is what one physician in our group is spending on production alone. You do not need to spend that to start. But you do need to spend something: either money or an enormous amount of your own time. Photography. Video. Copywriting. Social management. SEO/AEO. The infrastructure of a serious physician brand adds up faster than it looks. There is no high-quality brand built on zero investment. Know what you are committing to before you begin.
5. Expertise. Nobody taught you content strategy, audience building, platform algorithms, or how to write a hook that stops a scroll. That gap is real. It humbles a lot of brilliant physicians who assume clinical excellence translates directly to online credibility. It does not. The skills are different. The learning curve is steeper than it looks. The physicians who succeed online are not just good doctors. They are also students of communication. That is a second education. Go in with your eyes open.
The Only Brand That Works.
Not the most polished. Not the biggest budget. The most true.
The doctors who will lead the next decade of medicine are not the ones who figured out the algorithm. They are the ones who had something real to say, to a specific group of people who needed to hear it, and kept saying it.
Figure out what you stand for. Then go stand there. Loudly, consistently, and without apology.
Measure your impact in outcomes, not impressions. Educate with generosity. Share opportunities. Care for the people you serve and guide them ethically — with the full weight of clinical judgment behind every word.
Hippocrates understood this a few years ago ;) The physician’s duty was never just to treat. It was to heal, to teach, and to guide.
That has not changed. The screen is just a bigger room.
The world does not have enough doctors doing that. Be one of them.

Every week, the Longevity Docs WhatsApp group feels like a front-row seat to the future of medicine. Here’s what had doctors buzzing:
GLP-1s Are Stealing Joy. Does It Matter?
The weight comes off. The inflammation drops. The metabolic markers improve. But something else changes too. Some patients on GLP-1 agonists report a quiet flattening of life. Food stops being pleasurable. Hobbies feel distant. The drive dims.
One physician shared it happened to her personally at just 2.5mg of tirzepatide. She linked it to her COMT met/met variant, a genetic profile associated with slower dopamine clearance. She stopped the medication.
“N=1, but it was real. The anhedonia was bad enough that I didn’t want to continue.”
Another physician pushed back. For her, the clinical calculus is clear: optimize hormones first, check CYP2C19 metabolism, and consider adjunct options before attributing emotional blunting to the drug itself.
“Estrogen and testosterone status matter enormously here. I’ve seen patients feel completely different once we address the hormonal picture alongside the GLP-1.”
A third perspective: the new oral GLP-1 partial agonist entering the market may sidestep this entirely. Unlike full agonists, it reportedly preserves the drive for things that bring joy. The mechanism is different enough to warrant attention.
“It doesn’t kill motivation the same way. That’s a meaningful clinical distinction if it holds up.”
The deeper question no one has answered yet: are we selecting the right patients for these drugs? COMT variants, dopamine profiles, hormonal status. The era of prescribing GLP-1s uniformly may already be over for sophisticated longevity physicians.

No MBA? We got you! Launching Longevity Docs Growth.
Last week a physician in our group told me he’s been running his longevity practice for two years. Fully booked. No idea what his CAC is. No idea what his LTV is. Just working harder every month hoping the math works out.
That’s what Longevity Docs Growth is built to fix.
A business track for longevity physicians stepping into the next era of their practice and their life.
Whether you’re building from scratch, scaling what’s working, or expanding beyond the exam room: this track gives you the frameworks, the numbers, the playbooks, and the peers to do it faster and smarter than going alone.
Every session is built for longevity physicians, taught by longevity physicians and operators who have done it.
Who it’s for:
The physician ready to start their first longevity practice
The clinic owner ready to scale beyond where they are
The established doctor ready to diversify into speaking, products, partnerships, or platforms
The Sessions:
Session 1 — Strategy
“Build The Longevity Practice Blueprint” The 101 every longevity physician needs before they spend a dollar or see a patient.
Session 2 — Operations
“Operate Like a Formula One Team.” The operating system behind the world’s highest-performing longevity clinics.
Session 3 — Finances
“Know Your Numbers” ARR. CAC. LTV. CPA. The four numbers standing between you and a practice that actually makes you free.
Session 4 — Marketing
“Acquire Better Patients Faster” Stop chasing volume. Start attracting the patients who stay, pay, and refer.
Session 5 — Branding
“Build Your Brand Before You Need It” The physician who owns their name online never competes on price.
Session 6 Technology
“Download the Tech Stack” The exact tools the world’s best longevity clinics are running right now.
More than a generic MBA. Join us in Cannes. The Growth Track is included.
June 9–11. Cannes. You should be there.

GLP-1 Receptor Agonists
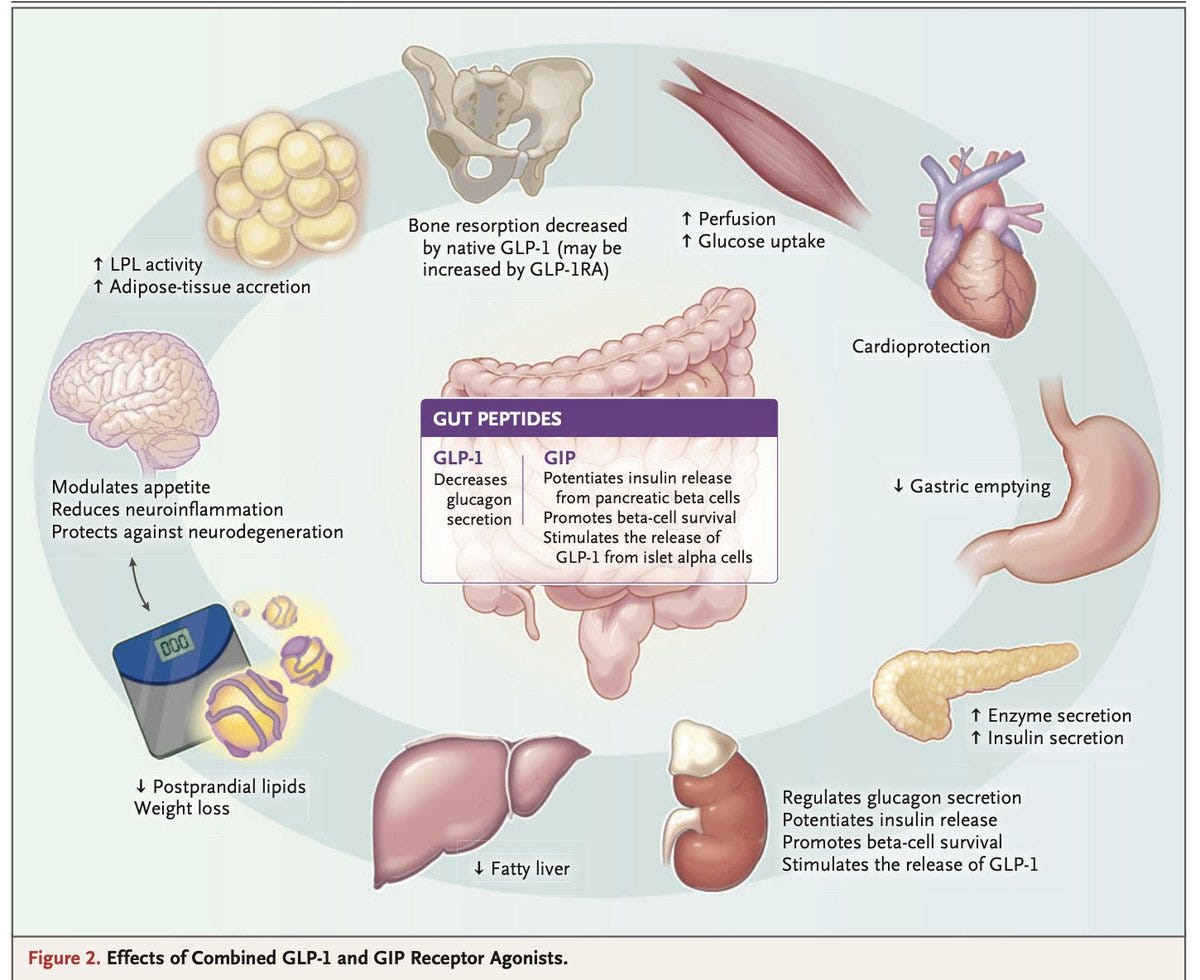
GLP-1 and dual/triple agonists (semaglutide, tirzepatide, retatrutide) are now first-line for type 2 diabetes and obesity, delivering up to 25% weight loss and meaningful HbA1c reductions. Large RCTs confirm significant cardiovascular and renal protection, independent of glucose control alone. Key concerns remain: muscle and bone loss with sustained weight reduction, weight regain after discontinuation, and long-term adherence data still limited to under 3 years. The frontier is expanding toward neurodegeneration, liver disease, heart failure, and cancer, but health equity and cost access remain unresolved. NEJM
Epigenetic Age Feedback & Lifestyle Change
Sharing personalized epigenetic age data with patients works: after one year, 72% felt healthier, 60% increased physical activity, and 63% improved health literacy. Not all epigenetic clocks are equal — massive variability across 14 models tested, with Zhang2019-BLUP selected as the most interpretable for patient-facing communication without triggering unnecessary anxiety. Behavior change was hardest in smoking and alcohol (only 3% and 26% improvement), confirming that deep habits need more than biomarker feedback alone. Community-based delivery through trusted local networks was a key driver of engagement and retention. Epigenonmes
Why it matters: Showing patients their biological age can be a powerful behavior change tools in your clinical arsenal. The clock you choose matters. Pick one your patients can understand and act on.
AI Scribes Reduce Clinical Time
Across 5 academic medical centers and 8,500+ clinicians, AI scribe adoption cut total EHR time by 13 minutes and documentation time by 16 minutes per 8-hour day, while adding roughly half a visit per week. Benefits were largest for primary care physicians, female clinicians, advanced practice clinicians, and those using AI scribes in more than half their visits. Notably, after-hours EHR time didn’t change significantly, suggesting AI scribes aren’t yet solving the burnout problem at its root. JAMA
Why it matters: AI scribes are a real but modest win — not a revolution. For longevity physicians running high-touch, complex consultations, the documentation burden is even heavier.

Welcoming the Certified Longevitydocs Candidates
This week, three physicians from across the world made the decision. They just joined our Certified LongevityDocs program to earn their CLD certification. Different specialties. Different continents. One decision.



Dr. Tiffany Moon (USA) is a board-certified anesthesiologist, entrepreneur, and cultural force who has built a platform that reaches far beyond the clinic walls. She understands that the future of medicine is not just about what happens in the exam room, it’s about who gets to shape the conversation. Her ability to bridge clinical credibility with mass reach is exactly the kind of voice longevity medicine needs more of. She’s bringing that energy here.
Dr. Paul Verrills (Australia) is a pain medicine and interventional specialist based in Australia, recognized internationally for his pioneering work in neuromodulation and advanced pain therapies. He represents something critical for this community: longevity medicine is not a US phenomenon. It is a global movement. Australia is on the map. So is everywhere else.
Dr. Gurmeet Soni Bhalla (India) is a longevity clinician, allergist, and Chief Medical Officer at Resolute, based in Bangalore, India. With over 25 years of clinical expertise in Allergy, Immunology, and Pediatrics, she is redefining preventive care by bridging evidence-based medicine with emerging insights in longevity and human performance.
These doctors didn't think about it. They are doing it. Get certified.

Every week, I track funding, FDA approvals, product launches, and breakthrough announcements shaping longevity medicine.
CARE
Hims & Hers Expands Personalized Digital Healthcare Platform
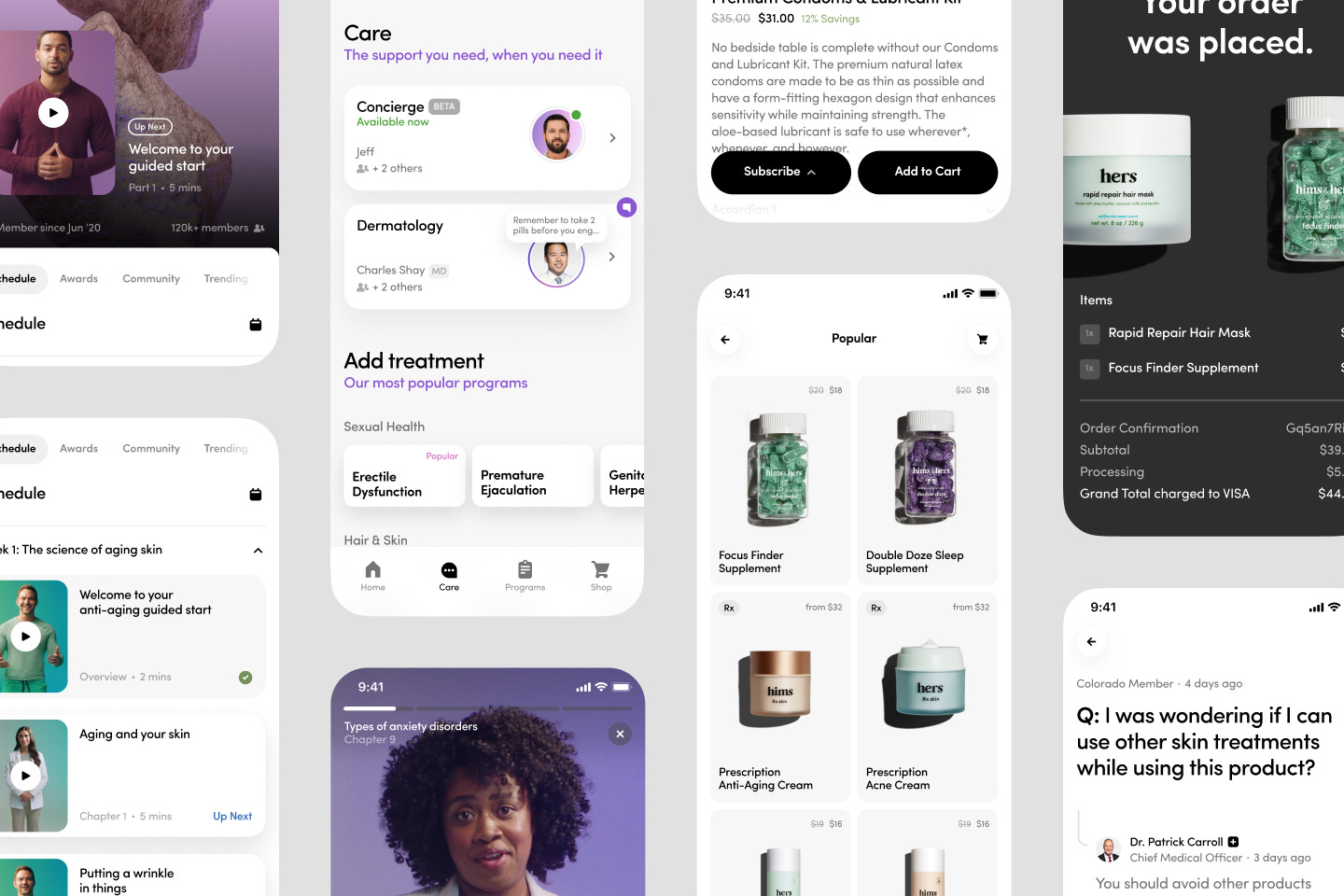
Hims is building a consumer-first digital healthcare platform that integrates diagnosis, treatment and fulfillment into a seamless, technology-enabled experience. Its model connects patients with licensed providers through telehealth, enabling personalized treatment plans supported by digital prescriptions, online pharmacy fulfillment and continuous clinical management.
───
AI & TECH
How A.I. Helped One Man Build a $1.8 Billion “Telehealth” Company
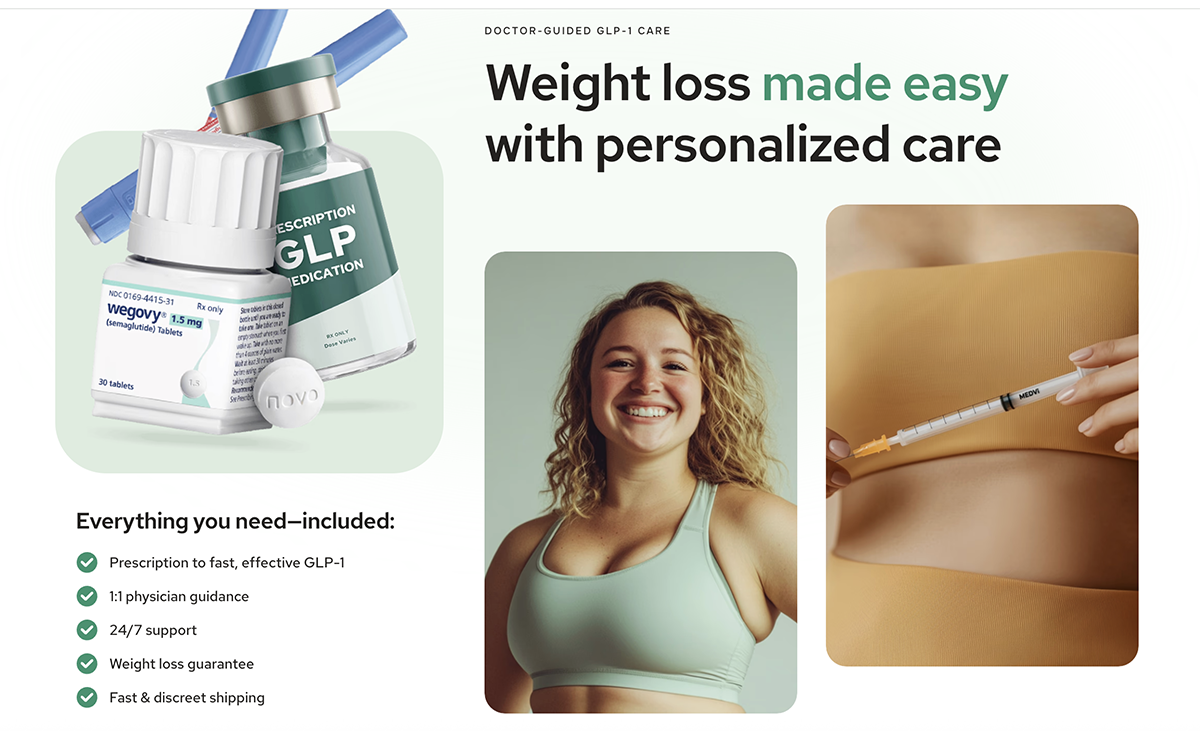
Matthew Gallagher built Medvi, a GLP-1 telehealth company, in two months with $20K and a stack of AI tools — Claude, ChatGPT, Midjourney, ElevenLabs — outsourcing medical, pharmacy, and compliance infrastructure to third-party platforms. Year one: $401M in revenue, 250K customers, 16% net profit margins. Year two on track for $1.8B. His only hire was his brother. No venture funding. No office.
Why it matters: A non-physician just built a $1.8B longevity-adjacent business by doing exactly what most doctors won’t — moving fast, using AI ruthlessly, and staying lean. The clinical infrastructure already exists. The technology already exists. The patients are already there. The only thing missing is the physician at the center of it. That’s the CLD. That’s Longevity Docs. The rails are being built whether we build them or not. The question is who controls them.
───
RESEARCH
Hallucinated citations are polluting the scientific literature. What can be done?
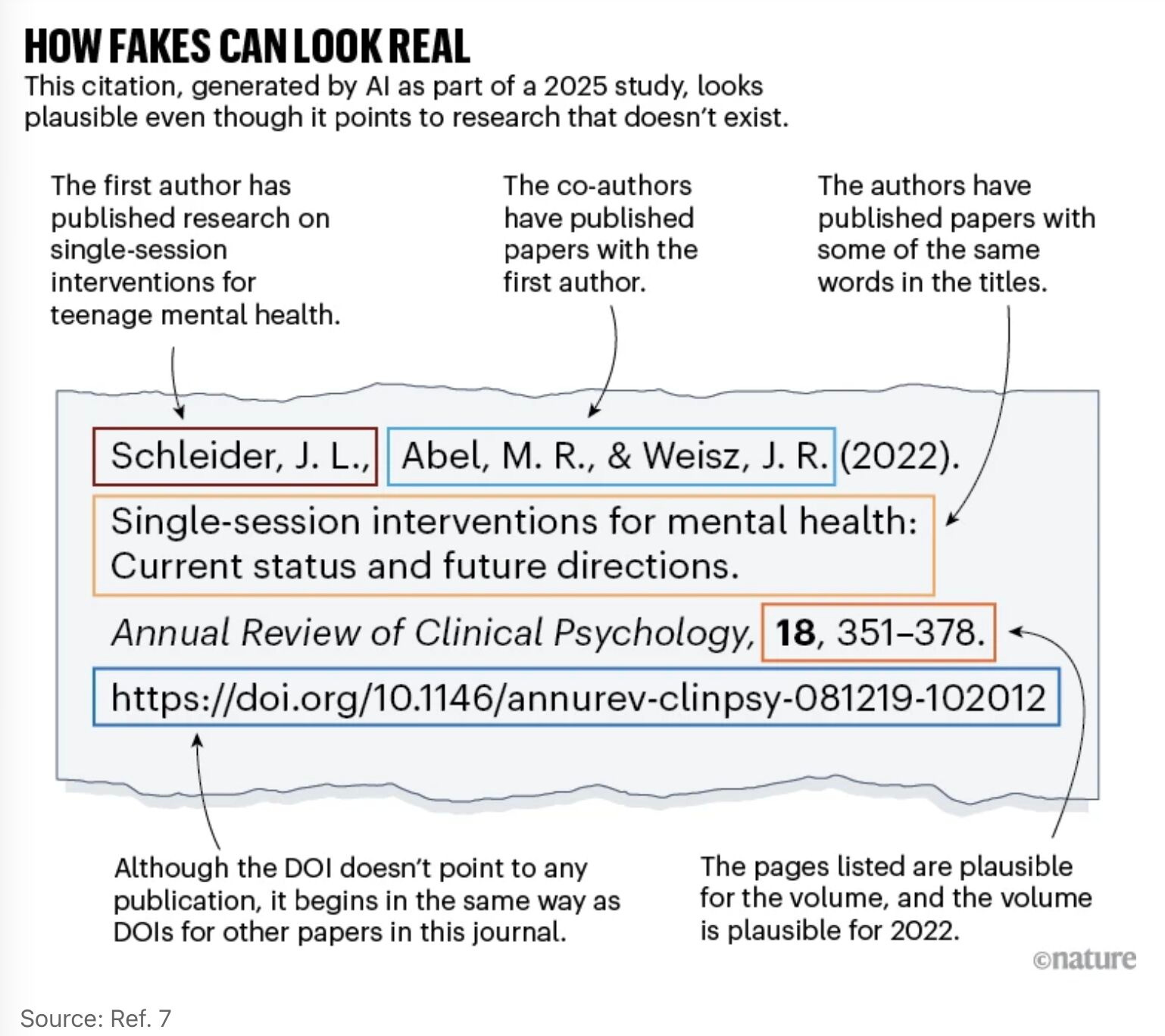
A Nature analysis estimates over 110,000 scientific publications from 2025 contain invalid AI-generated references, with 2.6% of papers in some fields carrying at least one hallucinated citation — up tenfold from 2024. AI models stitch together fragments of real papers into convincing but nonexistent “Frankenstein” citations, making them hard to detect even for editors. Major publishers are now deploying screening tools, but detection remains imperfect and the problem is almost certainly larger in smaller, less-resourced journals.
Why it matters: The longevity literature is already noisy. If AI-generated citations are polluting the reference lists of papers your patients and colleagues are reading, your clinical judgment and ability to evaluate evidence critically has never been more valuable. This is exactly why physician-led, evidence-graded intelligence — like what we’re building at Longevity Docs — matters.
PHARMA/BIOTECH
Japan Approves the World’s First Treatment Made With Reprogrammed Human Cells

Japan’s Ministry of Health, Labor and Welfare officially granted conditional and time-limited marketing authorization to two regenerative medical products derived from reprogrammed iPS cells, marking exactly 20 years since the creation of mouse iPS cells. These will be the world’s first practical application of iPS cell-derived products. Wired
Why it matters: Within five years, longevity physicians will be fielding patient questions about iPS-derived therapies. Understanding the regulatory pathway Japan is building now prepares you to lead that conversation.
CULTURE
Ipsos Report: Strategic Implications of the Longevity Medicine Revolution
Ipsos: longevity medicine is no longer wellness. it is pharma’s next frontier.
Ipsos identifies five strategic categories now shaping the longevity market: molecular therapies (senolytics, NAD+ boosters), system optimizers (microbiome, immune resilience), experimental preventives (gene therapy, cellular reprogramming), diagnostics (biological clocks, biomarkers), and repurposed drugs (GLP-1s, metformin). Big pharma, biotech, platform R&D, and DTC companies are all converging on the same thesis: medicine is shifting from treating disease to preserving healthspan.
Why it matters: The report confirms what longevity physicians already see in practice. The industry is moving from reactive to proactive. Pharma is repositioning existing assets around aging biology. Commercialization models are evolving beyond traditional HCP channels toward consumer-driven, prevention-first strategies. For longevity doctors, this means growing institutional validation, new diagnostic tools entering clinical workflows, and an expanding evidence base for interventions already being used in practice. The question is no longer if longevity medicine becomes mainstream. It is how fast.

Mastermind Replays Now Available
3 Masterminds. 3 topics reshaping longevity practice: AI & Tech, Peptides, and Hormones - featuring the dozens of faculty. Trusted by hundreds of physicians
If you weren’t in the room, this is your second chance.

Conferences
April 11 — A4M SpringFest · Miami
Jun 9–11 — Longevity Docs Cannes 2026”: Awards & Summit
Jun 29–Jul 1 — A4LI H-SPAN Summit · Washington, DC Longevity medicine meets regulation and policy.
Aug 24–28 — ARDD · Copenhagen, Denmark Where aging research meets drug discovery.
Oct 17 — Longevity Docs Skin Longevity Mastermind · New York, NY. Curated physicians. Deep science. One room.
TBA — Longevity Clinics Roundtables · Buck Institute Clinical practice meets research infrastructure.

The Home of Longevity Medicine
longevitydocs.™ is the world’s leading longevity physician community - 600+ doctors across 50 countries united by a single conviction: every doctor should be a longevity doctor. Founded by Dr. David Luu, the platform offers its members network, education, and experience with the mission to democratize longevity medicine.
Not a member yet? Join longevitydocs™
We’re a physician-only network. Curated. Vetted. Built on trust. If you’re committed to practicing longevity medicine with rigor, peer support, and shared standards → this is your community. Apply to connect with our team.
Longevity medicine is the personalized, evidence-based practice of modifying the root mechanisms of aging (biological, cognitive, and psychosocial) before they become disease, extending healthspan, not just lifespan. Using advanced diagnostics, precision interventions, and AI-enabled monitoring, it translates measurement into action across every medical discipline. Success is measured in functional capacity, vitality, and disease-free years.

Subscribe to the Longevity Docs Newsletter
Longevity medicine is moving fast. Every week, we bring you what matters: clinical insights, research signals, and perspectives from 600+ physicians across 50+ countries. One newsletter. Built for the physicians shaping this field.
Editorial Disclaimer:
Thank you for this . An inspiring read
Thanks for the inspiration on building a personal brand! I’ll start soon.