

Organ aging signatures ⎮ Long COVID ⎮ GLP-1RAs ⎮SGLT2i ⎮Mastermind Speaker Dr. Elizabeth Yurth
Your sneak peek into the world of Longevity Docs.

Hey Doc,
Welcome to this week's edition of the Longevity Docs Newsletter!
The buzz in the chat this week is all about long COVID—discover its impact and emerging treatments.
We'll also highlight groundbreaking publications on the aging signatures of organs using proteomics.
Plus, we're thrilled to announce that Dr. Elizabeth Yurth will be joining us in October to share her invaluable insights.
Grateful for this community 🙏
David Luu
🚨 Longevity Docs News
👋 Community: Welcome to our new members
Lucia Hue Fontaine, MD - Paris, France
Anil Bajnath, MD - Hanover, Maryland
Farid Zaer - Brisbane, Australia






Join a global network of 150+ physicians committed to evidence-based precision longevity medicine.
🎤 Events
Dr. Elizabeth Yurth will speak at the Longevity Docs Mastermind NYC on October 5-6

As a double board-certified physician in Physical Medicine & Rehabilitation and Anti-Aging/Regenerative Medicine, Dr. Yurth has more than 30 years of clinical experience and continues to stay at the forefront of orthopedics, cellular medicine, regenerative medicine, and the future of aging.
Dr Yurth is the Co-Founder and Chief Medical Officer of Boulder Longevity Institute, where she has been providing Tomorrow’s Medicine Today to her clients since 2006. Dr. Yurth obtained her Medical Degree from the University of Southern California Keck School of Medicine, completed her residency at the University of California – Irvine, and her Fellowship in Sports and Spine Medicine from Stanford-affiliated Sports Orthopedics and Rehabilitation (SOAR) in Palo Alto, CA.
Along with her 30 years as a practicing orthopedist specializing in sports and spine medicine, Dr. Yurth has made it her mission to learn and share the latest scientific research on how to truly heal the body at the cellular level. She is Fellowship trained in Anti-Aging, Regenerative, and Cellular Medicine and has completed +500 hours of CME training focused on Longevity, Nutrition, Epigenetics, Bioidentical Hormone Replacement Therapy, Regenerative Peptide Treatments, and Regenerative Orthopedic Procedures.
💬 Buzz in the Chat
Discussion on Long COVID
As longevity docs we need to take COVID, recurrent exposures to any form of spike protein, and Long COVID VERY seriously.
We are seeing a tsunami of neurodegenerative, cardiovascular and autoimmune diseases, as well as vascular/thrombotic conditions, malignancies, and metabolic disorders play out before our very eyes and it only stands to get worse as the virus continues to mutate, with no seasonality, and becoming even more transmissible (I will share that recent paper). People will now continue to be infected multiple times per year- studies showing that even ONE asymptomatic or mild case can lead to a 5 point drop in IQ- how can we sustain this?
While of course best practices is taking an EBM approach, we can’t stop doctoring. This is a beast of a disease and continues to evolve at lightening speed. We will have to adapt quickly as well, so waiting around for the next double blind placebo controlled trial to emerge is not going to get us very far and leave millions disabled or dead.
My research consortium has now identified 26 host cell receptors that spike protein can bind to gain entry into the cell. No wonder it’s so infectious and can do so much damage!!
This has massive health implications like we have never seen in the history of medicine. This is NOT the Spanish flu, and I am sorry and don’t mean to be offensive, but anyone that compares it to that or any other virus has NOT done their homework and has a poor understanding of the science.
My self and my group, based on the scientific data we have amassed in the past 4 years, along with clinical data we have been capturing over the past year and a half, do believe that there are specific advanced biomarkers, testing and imaging studies that help aid in diagnosis and treatment. However, I would love to create a consensus panel with the help of anyone in this group that allows us to not only help identify Long COVID patients, but those that are also “in trouble” due to repeated exposures or that may have a “form of Long COVID”, from spike protein damage, but just don’t realize it (i.e. sudden onset of uncontrolled HTN).
Pill for every ill” approach needs to be abandoned, especially when over 300 different biochemical pathways are effected (~ 80 being oncogenic). So using targeted drug therapy will get us nowhere. We need to use natural compounds and repurposed drugs collectively what we know can hit upstream and multiple pathways at once!
Treatment MUST focus around the root cause:
-Remove the spike protein and address persistent virus!!
Then go downstream to address post- inflammatory changes/pathology-
-Restore health and balance to the gut microbiome- this is destroyed post- COVID
-Improve mitochondrial reserve and function
-Restoration of cell membrane health
-Address the glycocalyx, loss of elastin, and restore endothelial flexibility
-Restore and repair the BBB and the glymphatic system
-Clear autoantibodies
And lastly, focus hard on prevention and/or squashing viral replication FAST if infected!!
My apologies for rambling on- I would love to share my knowledge, show you all what I have learned, and how my group has been addressing this. We also have some emerging studies with results expected in the next 90 days or so.
I am humbled to be part of such an astute group of brilliant, hard working physicians, and am blessed to learn from each of you everyday. I would be honored to return that favor in whatever small or big way I can!
You are incredible! I especially appreciate how you are looking this problem diagnostically and therapeutically through the lens of cell signaling.
A related question- if this infection is now endemic and cumulative exposure has negative effects- is there anything you recommend in the vein of prevention/prophylaxis?
I’m sure many of us have our own “immune protocols” that we run empirically (I personally focus on TA1, zinc, vitamin D, ketone esters) , but we don’t have the data/insight you have.
Appreciate all that you have shared and all that you are doing!
Good morning, the recent MENSA essays indicate that these are indeed, persistent, viral infections in the long Covid patients. We have to get the spike protein out of the body however, it got in there and we have to stop replication of the spike proteins. However, that got in there I think that the research group identifying microbiome alterations and bacteriophage actions of infection are going to be proven correct here. But there are other viral reservoirs that we see and other viruses and so I think we need to think of this in terms of combination therapy for infections. One thing is clear ritonavir is a pretty toxic molecule, so I don’t think PAX lovid should be anywhere around this. For prophylaxis you need to think about the infection cycle and the replication cycle acting on those early with medication‘s. That are not going to give you pancreatitis or spur, foam cell growth or endothelial inflammation will be essential. Alternatively, you could just have everyone walking around in PAPRs. There are lots of suggested vitamins and I think the data are soft on most at best. I do think one thing will be essential here and that is reversing any immunosenescence that you have going on already. And I think prophylaxis as a whole is going to be exceedingly tough unless you were willing to commit yourself to good respiratory hygiene.
This is what I am talking about- a beast…..
This is exactly why I do not do Orthobiologics with PRP/Stem Cells for 90 days post infection. I am also seeking screening preprocedure.
It really does hit all hallmarks of aging. Most have been reported. We need a best method for diagnosing this damage and then treating.
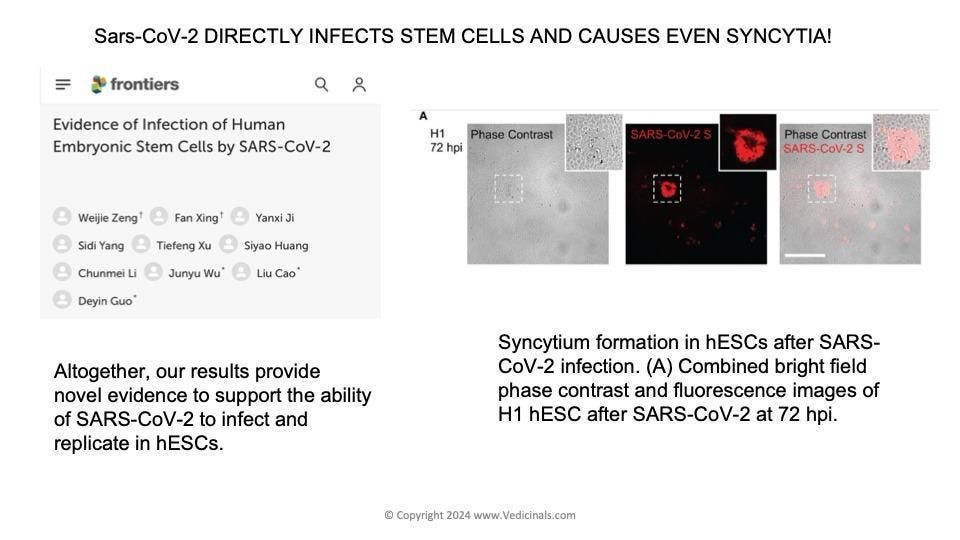
Yea, but these syncytia don’t go away- they need to be “taken out”- waiting 90 days may not make a difference unfortunately…..
I suspect thats why TA-1 might be the best prophylaxis we have. Unlike various vitamins, TA-1 targets the exact mechanisms you mention via signaling modulation.
SGLT2 inhibition eliminates senescent cells and alleviates pathological aging
These findings suggest that inhibition of SGLT2 has an indirect senolytic effect by enhancing endogenous immunosurveillance of senescent cells.
Nature Aging - Recommended by Dr. Sajad Zalzala
GLP-1 receptor activation inhibits Toll-like receptor agonist-induced inflammation
Glucagon-like peptide-1 receptor agonists (GLP-1RAs) exert anti-inflammatory effects relevant to the chronic complications of type 2 diabetes.
Cell Metabolism - Recommended by Dr. Steven Murphy
Organ aging signatures in the plasma proteome track health and disease
We introduce a simple and interpretable method to study organ aging using plasma proteomics data, predicting diseases and aging effects.
Nature - Recommended by Dr. Mark Gordon

🌐 In the News
Think You Will Live to 100? These Scientists Think You’re Wrong
Vitalia CEO Niklas Anzinger on the longevity city success story
🗓️ Events & conferences
👉 Longevity Docs Mastermind: NYC - October 5,6
LiveLong Summit: Los Angeles - August 3,4
Cellular Senescence - the Road to Immortality : Novato - August 12
ARDD: Copenhagen, Denmark - August 26,30
Cannes Longevity Festival: Cannes, France - June 25,27 2025
About Longevity Docs
Longevity Docs is a highly-vetted membership network dedicated to physicians pioneering precision and evidence-based practices in longevity medicine.