

Longevity Tour: 50 Lessons from 5 Cities
Issue 74: The front page of longevity medicine - curated by doctors, for doctors.

Hey Doc,
I’m late for the Sunday newsletter. Six days. Five cities. Lab visits, physician roundtables, panels, research sites, founder sessions, top executive rooms. With the people actually building the future of longevity medicine.
I tried to write this on the red-eye back from San Francisco. What I saw/heard deserved more than a rushed recap. I could write a book about it (In fact, I asked Google Ai studio to generate this cover while I was thinking about it.)









Three years ago, these conversations barely existed. Today, they’re everywhere. And they’re no longer speculative. They’re clinical, technical, ethical, political, and operational.
This is no longer a trend. It’s the formation of a new medical discipline.
Longevity medicine today feels like emergency medicine in the 1970s. Early. Undefined. Debated. But inevitable.
The science is accelerating. Capital is here. Patients are already asking their doctors for protocols
Now the responsibility shifts to the medical community.
The real question is no longer if longevity medicine will exist.
It’s how we collectively build the workforce, the standards, the data, and the trust to make it real.
What follows are 50 lessons from 5 cities in 6 days: Paris, London, San Francisco, Novato, and New York: organized into 10 chapters on how longevity medicine is actually being built.
Dr. David Luu
Founder, longevitydocs.™, the world’s largest physician network in longevity medicine, serving 600+ vetted physicians across 50+ countries. We unite physicians, industry, and institutions to build the trusted global infrastructure that makes longevity medicine the new standard of care.
Longevity medicine is the personalized, evidence-based practice of modifying the root mechanisms of aging (biological, cognitive, and psychosocial) before they become disease, extending healthspan, not just lifespan. Using advanced diagnostics, precision interventions, and AI-enabled monitoring, it translates measurement into action across every medical discipline. Success is measured in functional capacity, vitality, and disease-free years.

Each week, I try to explore one idea that could advance longevity medicine and hopefully support physicians in bringing it to life.
50 Lessons from the Longevity Tour
5 cities, 6 days, and the birth of a new medical discipline
If I had to write a book about this longevity tour, these would be the chapters:
Chapter 1: The Discipline Is Forming
1. Longevity medicine mirrors emergency medicine in the 1970s: early, undefined, debated but inevitable.
2. Three years ago these conversations were speculative. Today they are clinical, technical, and operational.
3. The field has reached an operational inflection point. The constraint is no longer innovation or capital. It is trained physicians.
4. In 2024, conservative physicians shifted from “should we” to “how do we.” Testing and EMRs recommendations now dominate the discussion.
5. What feels like a wellness trend today will be standard practice within 15 years.
Chapter 2: The Science Has Matured
6. The biology of aging must be taught in medical school. Only three institutions are piloting curricula for 2026.
7. Epigenetic clocks are ordered more frequently than annual physicals for patients over 40 in early adopter clinics.
8. Lifestyle remains the foundation, but biomarkers now drive precision in months, not decades.
9. Longevity physicians must publish outcomes, even with small cohorts. Legitimacy requires data.
10. GDF15, organ clocks, and proteomics are moving from research into clinical reality in 2026.
Chapter 3: The Workforce Is the Bottleneck
11. The core science of aging is now established. The remaining problem is delivery.
12. An estimated 50,000 trained longevity physicians are needed in the US by 2030. Fewer than 2,000 exist today.
13. Peer judgment delays adoption more than regulation. Cultural fear costs the field 2–3 years.
14. Social media is now essential for physician education and public trust.
15. Conservative cardiologists and endocrinologists entering the field are raising clinical credibility fast.
Chapter 4: Infrastructure Over Innovation
16. Longevity medicine will not scale through clinics alone. It requires shared infrastructure.
17. Certification is not education alone. It is delivery infrastructure: protocols, peer review, documentation, liability.
18. Longevity physicians require multidisciplinary training across diagnostics, therapeutics, AI, research, ethics, and operations.
19. The field needs real-time market intelligence connecting physicians, institutions, and industry.
20. Education builds workforce. Community builds standards. Research builds legitimacy. Media creates demand.
Chapter 5: Legitimacy Determines Survival
21. Innovation without legitimacy will be stopped by regulators, insurers, or one high-profile adverse event.
22. A single off-label scandal could trigger federal intervention and stall the field for a decade.
23. A universal definition of longevity medicine is mandatory for institutional recognition.
24. Primary care physicians must be partners, they are the future longevity doctors
25. Documentation is both patient care and legal defense.
Chapter 6: The Economics of Practice
26. Patient churn is the biggest operational risk. Retention determines survival.
27. The average longevity clinic could break even at ~150 patients and scales profitably at 250+.
28. Patient acquisition could costs $2,000–$5,000 with lifetime value of $8,000–$20,000.
29. Churn peaks at 18 months when biomarker improvements plateau.
30. Payment processors could be hostile to longevity medicine.
Chapter 7: Beyond Disease Management
31. Longevity medicine is becoming the next evolution of general practice
32. Women and children‘s longevity are the most underbuilt frontier in clinical medicine.
33. Menopause is a medically ignored 10-year intervention window.
34. Beauty and aesthetics are the front door to longevity medicine financially.
35. Pediatric longevity will reshape population health, but regulation does not exist yet.
Chapter 8: Trust Is Everything
36. In 2025, trust matters more than innovation.
37. Off-label, functional medicine, and experimental care must never be blurred without transparency.
38. Physicians should compete on outcomes, not social media following
39. Public attacks on critics weaken the entire field.
40. Belief and behavioral changes are real clinical forces that must be acknowledged.
Chapter 9: The Global Market Reality
41. Longevity is accelerating because demand, capital, science, and tech are converging at once.
42. The U.S. led early because of a broken healthcare system and venture capital risk tolerance.
43. China and Middle-East are the next growth engines with government-backed longevity investment.
44. Biology and clinical evidence are becoming the new luxury market.
45. Longevity is the only healthcare market with seven billion potential customers.
Chapter 10: AI Is the Accelerant
46. AI is becoming the infrastructure of medicine, not a tool on top of it.
47. The AI tools working today: ambient scribing, biomarker interpretation, patient messaging.
48. The AI tools failing adoption: complex multi-omic platforms that cannot be explained or billed.
49. The biggest AI barrier is malpractice fear, not capability.
50. Population-scale biological age tracking is now technically feasible. Health systems are not ready yet.
The Responsibility Is Ours
What became clear across every city is this:
Longevity medicine is no longer at the edges of medicine. It is moving toward the center.
But this transition will not happen through innovation alone. It will happen through education, standards, research, ethics, and real-world care models that actually work.
The science is accelerating. The capital is flowing. The public is ready.
Now the responsibility shifts to the medical community.
To train the next generation.
To publish the data.
To set the standards.
To work together across institutions.
To move from discussion to coordinated action.
The science of longevity is solved. The remaining problem is delivery—and delivery is a workforce problem.
Longevity medicine is not about adding years at the end of life. It is about redesigning the practice of medicine across an entire lifetime.
The field is taking shape. The pace is accelerating. And the doctors who master it now will define it for the next 50 years.
Building the Workforce
The bottleneck is real. The opportunity is now.
Longevity Docs trains physicians with the certification, protocols, peer networks, and practice infrastructure required to deliver longevity medicine safely and profitably.
If you are a physician ready to integrate longevity medicine into your practice, learn how we empower physicians to be longevity medicine ready.

Every week, the Longevity Docs WhatsApp group feels like a front-row seat to the future of medicine. Here’s what had doctors buzzing:
Payment Processing Challenges
Square suddenly booted longevity clinics for processing prescription medication payments when card-not-present, creating an operational emergency across the network. The community rallied with solutions: consultant (specialized for longevity clinics), Stripe with BAA, or creative workarounds. This reflects a broader industry challenge as payment processors struggle to categorize emerging longevity medicine practices.
“Welcome to the club. Good luck many others feel the same.” - Dr. P
“This is a huge issue and anybody who hasn’t run into it...depending on what you do probably will.” - Dr. Y
Key Takeaway: Payment infrastructure is actively hostile to longevity medicine. Build relationships with specialized processors now before you’re deplatformed mid-practice.
GlycanAge & Hormone Optimization
GlycanAge testing sparked a masterclass from Dr. R on using it clinically: the most powerful lever isn’t lifestyle, it’s estradiol exposure over the prior 3 months. Perimenopausal women can age 10 years in one year without optimization, but proper HRT can reverse GlycanAge by 15-20 years.
“The most important factor impacting GlycanAge is the previous three months of estradiol exposure.”
“I routinely lower patients in ages by 15 to 20 years over the course of a year by increasing their estrogen level to an optimal level in both males and females.”
Key Takeaway: The Glycan Mature sub-test could reveal if a patient is estrogen-responsive, making this actionable beyond generic “reduce inflammation” advice.
Mitochondrial Testing Anyone?
The debate over which mito tests actually matter got intense: MitoSwab/Mitome shows high variability in split samples, MeScreen measures live cellular energetics, and everyone agrees single tests are insufficient. The consensus? Mitochondrial assessment requires multimodal approaches (Acylcarnitine, Lactate/Pyruvate, OATS, oxidative stress), and the field desperately needs standardized protocols and education.
“Mitochondria are the sentinel for cellular dysfunction.” - Dr. M
“The problem is I can get repetitive blood pressure to get averages. I can’t do that with mitoswab...and so I don’t think single testing is useful enough.” - Dr. Y
Key Takeaway: Mitochondrial testing is critical but chaotic: no single test is reliable enough. Use multiple modalities, trend over time, and invest in deep metabolic knowledge before ordering expensive tests you can’t interpret.
Not a member yet? Join the debate in the WhatsApp group
Longevity Docs is a highly vetted, invitation-only community for physicians shaping the future of longevity medicine. Apply to connect with our team.

Each week, I highlight studies that could shape the future of longevity medicine.
Clinical evidence for the use of NAD+ precursors to slow aging
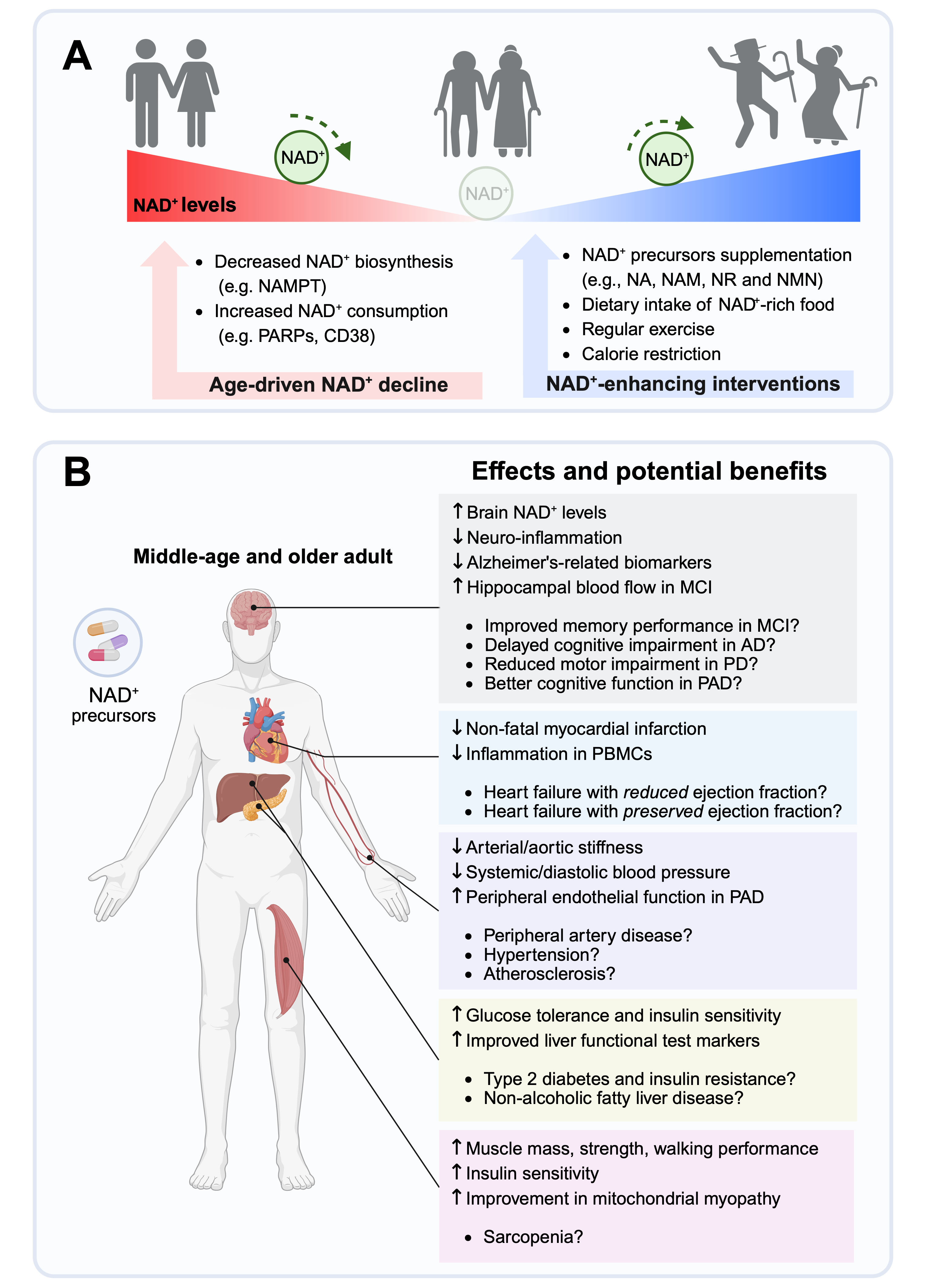
NAD+ precursors (niacin, NAM, NR, NMN) are generally safe in humans and reliably raise circulating NAD+, but effects are modest and context-dependent.
Small trials show early signals in vascular health, insulin sensitivity, muscle performance, inflammation, and skin cancer prevention, but results are inconsistent.
There is no strong evidence yet that NAD+ supplements broadly “slow aging” or improve hard outcomes like mortality, major CV events, or dementia. Geromedicine
For longevitydocs: For now, NAD+ precursors are best viewed as experimental adjuncts layered on top of proven longevity interventions.
Risk of Cancer with GLP-1RAs
GLP-1RAs may have little or no effect on colorectal, esophageal, liver, gallbladder, ovarian, or endometrial cancer; multiple myeloma; or meningioma (low certainty). The effect on gastric cancer is very uncertain. Results were consistent in sensitivity analyses of trials with low risk of bias and studies of semaglutide or tirzepatide and across subgroups stratified by follow-up duration, population, GLP-1RA class, weight loss profile, dose, and duration of action. Annals of Internal Medicine
For longevitydocs: GLP-1RAs may have little or no effect on risk for obesity-related cancers. Longer-term studies are needed to clarify potential risks or benefits.
Associations between sleep and physical activity
In this Communications Medicine large-scale analysis, they observed that only ~13% of people consistently achieve both 7–9 hours of sleep and >8,000 steps/day, while ~17% are short-sleeping and sedentary. They also observed that sleep duration and quality have a stronger impact on next-day physical activity than physical activity has on subsequent sleep.
For longevitydocs: sleep should obviously be treated as a primary intervention and objectively tracked as a core pillar of every longevity protocol
Thymus regeneration in Axolotl
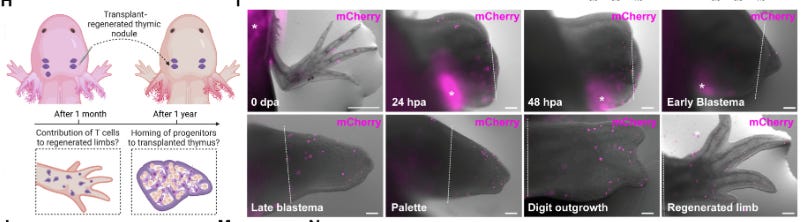
Thymus regeneration was associated with restoration of morphological and transcriptional features. Whereas the key mammalian thymic transcription factor FOXN1 was dispensable for thymus regeneration, single-cell transcriptomics identified the growth factor midkine as a likely driver. Future studies in axolotls could inform new therapeutic approaches for promoting thymus regeneration.
For Longevity Docs: Thymus/immune regeneration via MDK/BMP-like pathways is a serious future target for “immune age” reversal.

Every week, I track funding, FDA approvals, product launches, and breakthrough announcements shaping longevity medicine.
RESEARCH
Mini Mitochondria Factories
Texas A&M researchers created “mini mitochondria factories” by using nano-particles (“nanoflowers”) to supercharge stem cells so they produce and donate twice as many mitochondria to damaged cells. The approach leverages natural mitochondrial transfer and could impact diseases of aging like Alzheimer’s, diabetes, fatty liver, and muscular dystrophy. The method is still preclinical, with animal testing starting soon and long-term human safety unknown.
For longevitydocs: This is another strong signal that mitochondrial repair and transfer (not just boosting) may become a future therapeutic pillar for aging and immune-metabolic decline.
AI/TECH
Can AI Look at Your Retina and Diagnose Alzheimer’s?
In this WIRED’s interview, Eric Topol says: “This is a unique moment in medicine. Part of it is because we have multimodal AI, but part of it is because we have new layers of data. We never had organ clocks, which track the pace of aging for every organ of your body, including your immune system. We never had biomarkers like p-tau217, which tells us about our risk of Alzheimer’s 10, 15, even 20 years in advance. The biggest jump in recent biomedicine is the ability to quantify metrics of aging.”
For longevitydocs: We will soon be able to measure the drivers of aging continuously, not just with one-off tests. Longevity medicine is shifting to real-time tracking with AI-driven interpretation.
POLICIES
FDA announces TEMPO, a new pilot to tackle chronic disease with tech

FDA launched TEMPO, a pilot to fast-track proven digital health devices for chronic disease using real-world home monitoring data. Built with the CMS, it supports cardio-metabolic, musculoskeletal, and behavioral health through remote, tech-enabled care at home.
For Longevity Docs: this validates the shift to “Home as a Longevity Hub”: continuous monitoring, data streaming, and AI-driven care starting where patients live.

VEGAS TABLE | DECEMBER 13, LAS VEGAS

The real conversations don’t happen on stage. A private dining room. 15 physicians.
longevitydocs.table is our jeffersonian-style dinner where leaders in longevity medicine speak openly about growth, ethics, business, risk, and the future we’re building together. After Miami, NYC, Boston, London, and San Francisco - we close the year at Mylos at The Venetian this saturday.
I’ll be there. Under 5 seats left.
AI & TECH MASTERMIND | JANUARY 31, NYC
We’re bringing together 150 longevity physicians building AI-powered longevity practices.
If you’re still figuring out which AI tools are HIPAA-compliant, how to integrate wearables into clinical decisions, or whether proteomics is ready for practice, this is where you get answers from physicians already doing it.
What we’re covering:
Next-gen biomarkers (proteomics, epigenetics, multi-omics)
Wearables and continuous monitoring: clinical-grade vs. wellness theater
NeuroTech and brain aging protocols
Performance metrics that track biological age
AI imaging that catches what radiologists miss
Tech stacks that actually work (EMR integration, dashboards, APIs)
Clinical workflow tools: triage, documentation, protocol generation
AI-powered practice growth without physician burnout
The debate: frontier tech vs. what’s ready now
Your Monday morning action plan: 90-day implementation roadmap
Small group. Curated. Limited to 150 Physicians only.
VIP (50 spots) - Includes private dinner with speakers
In-Person (limited) - Full access to all sessions and networking
Virtual - Live-stream and replay for those who can’t travel
Early-bird ends December 15.

The world’s largest physician network in longevity medicine
longevitydocs.™ is the world’s largest physician network in longevity medicine, serving 600+ vetted physicians across 50+ countries. We unite physicians, industry, and institutions to build the trusted global infrastructure that makes longevity medicine the new standard of care.

Our Pioneering Approach: Uniting Science, Clinical Practice, and Culture
Professional Network
Global Longevity Community: A curated community of leading longevity physicians fostering peer learning, clinical collaboration, and professional growth
Medical Education
Certified longevitydocs.™ (CLD): The first structured, physician-led clinical curriculum for longevity medicine - comprehensive, evidence-based, and practice-ready.
Clinical Research
Longevity Research Network: Clinical research infrastructure enabling rapid generation of real-world evidence across the Longevity Docs network.
Cultural Experiences
Global Events: From Cannes to New York, our Summits, Awards, Masterminds, and Jefferson Dinners convene top researchers, clinicians, investors, and government officials to shape longevity medicine’s growth, investment, and policy.
Intelligence
Strategic Insights: Weekly syntheses of scientific breakthroughs, clinical best practices, business signals, and global market analysis for Fortune 500 companies - the industry’s trusted source of intelligence.
Not a member yet? Longevity Docs is an invitation-only network of 600+ physicians shaping the future of longevity medicine through clinical collaboration, certification, and global events.
Subscribe to the Longevity Docs Newsletter
Stay connected with a global network of 500+ physicians in 50+ countries advancing longevity medicine. Get evidence-based insights, clinical updates, and exclusive access to the community shaping the future of longevity care.
Newsletter Disclaimer:
I just wrote a new article on this space - love your thoughts on it! https://open.substack.com/pub/springfutures/p/who-gets-more-time
Incredible tour synthesis. The comparison to emergency medicine in the 1970s is spot-on, especially the operational inflection point where the constraint shifts from innovation to workforce. The 50k physician gap by 2030 versus 2k today really underscores why certification and shared infastructure matter more than research breakthroughs at this stage. Payment processor hostility is also a signal that systemic legitimacy lags far behind clinical readiness.