

Launching the First Longevity Clinical Trial Network
Issue 70: The front page of longevity medicine - curated by doctors, for doctors.

Hey Doc,
Every Sunday I write this newsletter with one mission: to empower longevity physicians.
This week I’m particularly excited to announce another layer of our ecosystem: research.
Our path has been deliberate: Community → Events → Education → Research.
Each step builds the infrastructure to democratize longevity medicine and make it the new standard of care.
Today we’re launching longevitydocs.research
This is the first physician-powered Clinical Trial Network in longevity medicine.
First up: helping Mount Sinai recruit physician investigators for their XPRIZE Healthspan 2025 trial testing Rapamycin, Metformin, GLP-1s, and Spermidine with validated endpoints.
Healthy Sunday!
Dr. David Luu - Founder, longevitydocs.™
PS: I designed this cover, inspired by the beauty and complexity of human connectivity, a reminder that every pathway in the body, like in longevity medicine, belongs to a larger system working in harmony.

Each week, I try to explore one idea that could advance longevity medicine and hopefully support physicians in bringing it to life.
Why we are launching the first Longevity Clinical Trial Network Powered by Physicians
Longevity medicine is emerging fast. Yet as the field grows, so does the need for validation.
Today, most interventions are supported by small studies, animal data, or anecdotal success.
Randomized clinical trials, while essential, remain costly, slow, and limited by infrastructure.
Traditional health systems aren’t designed for longevity research: too few investigators, too few patients, too many barriers between innovation and evidence.
That’s why we’re launching longevitydocs.research the first Clinical Trial Network in longevity medicine, powered by physicians. Our mission: bring more evidence to the field and make longevity medicine the new standard of care.
With 600+ physicians worldwide already practicing longevity medicine, we’re uniquely positioned to bridge science, practice, and community. longevitydocs.research connects physicians, academia, and innovators to create a new model: decentralized, data-driven, and clinically grounded.
Our first step: partner with academic institutions to help recruit principal investigators and patients for ongoing studies. Next, we’ll collaborate with innovators, from biotech to diagnostics, supplements, and wearable tech, to validate their interventions in real-world settings. Over time, we’ll empower physicians to run their own studies, contribute to longitudinal registries, and build an ever-growing base of real-world evidence.
We believe this model can redefine how research is conducted in longevity medicine: faster, more inclusive, and closer to the patients it’s meant to serve.
We’re starting by helping Mount Sinai recruit physician investigators for their XPRIZE Healthspan 2025 trial, testing Rapamycin, Metformin, GLP-1s, and Spermidine with validated healthspan endpoints.
Mount Sinai XPRIZE 2025 Healthspan Clinical Trial
Mount Sinai invites Principal Investigators to participate in the upcoming XPRIZE Healthspan 2025 clinical trial, a landmark initiative to quantify and optimize biological aging through immune, muscle, and cognitive outcomes.
Objective
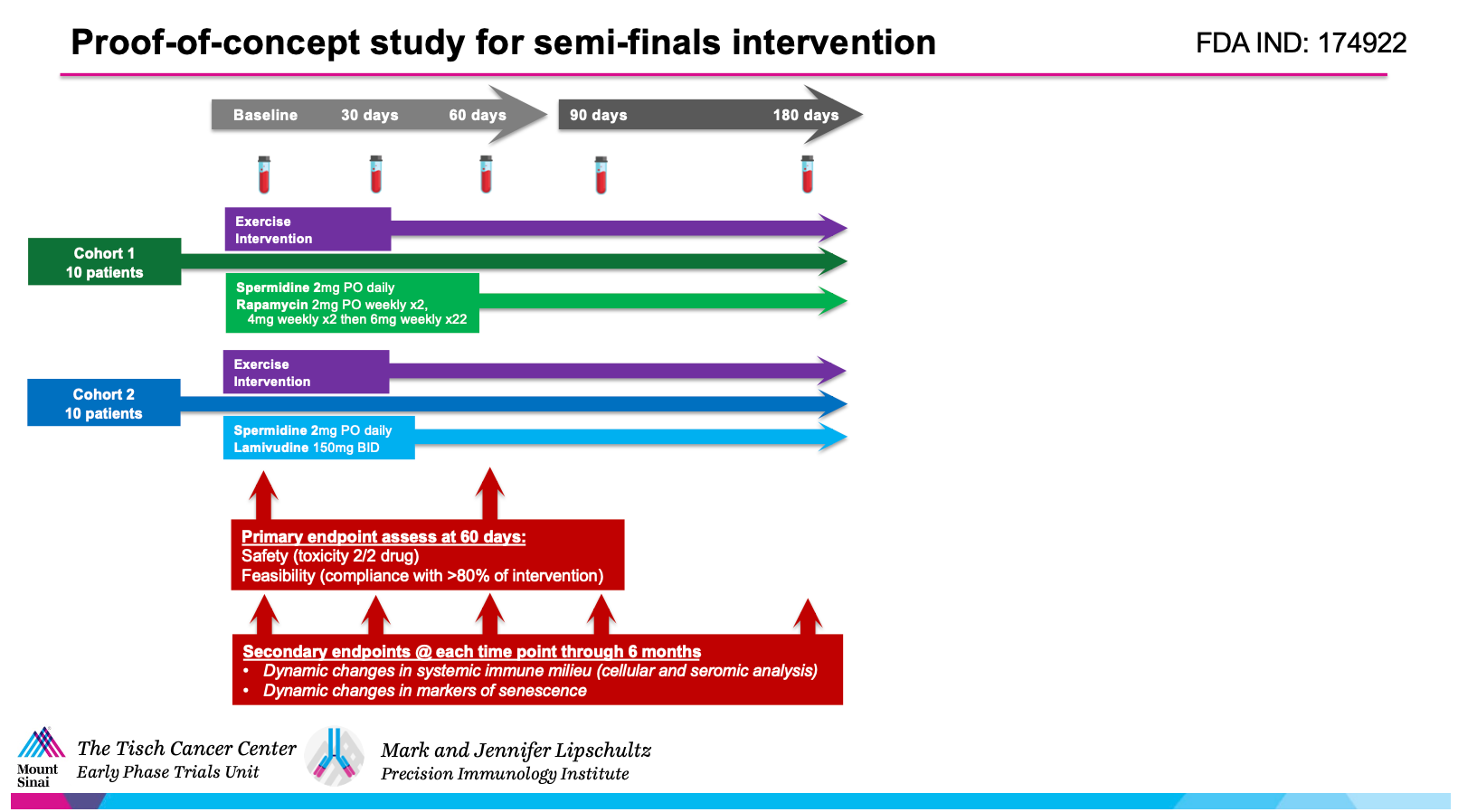
To characterize the immunodynamic effects of widely used longevity interventions, including Spermidine, Rapamycin, Metformin, and GLP-1 agonists.
The study will generate real-world evidence on how these interventions modulate aging trajectories, while accelerating the transition from anecdote to evidence in longevity medicine.
Primary Outcomes
Validated Healthspan Improvement defined by personalized response thresholds across three key systems:
Muscle Function: endurance capacity (peak VO₂), lower body power, muscle mass (D₃-creatine dilution)
Cognitive Function: executive function, processing speed, working memory
Immune Function: ex vivo naïve immune response to novel stimuli, immune cell composition (IMM-AGE signature)
5 Reasons to Become a Physician Investigator
Pioneer evidence-based longevity medicine to help establish the protocols that will define the field
Offer your patients research-grade interventions with institutional backing
Build academic credibility through publications and contribute to the scientific foundation of longevity care
Get compensated for your participation: both PI fees and patient enrollment incentives provided
Minimal time commitment: academic partners handle IRB, biomarker analytics, and infrastructure
Physician with active patient panels apply now. Limited seats

Every week, the Longevity Docs WhatsApp group feels like a front-row seat to the future of medicine. Here’s what had doctors buzzing:
Microbiome Testing Debate
What’s everyone’s favorite GI biome testing? So many panels and lots of controversy
The responses revealed a fascinating split:
The Accuracy-First Camp prefers tests using culture plus PCR methodology for reliability. But several physicians flagged a critical issue: false-positive H. pylori results creating unnecessary treatment.
The Comprehensiveness Camp wants maximum data despite the “overwhelm.” As one doc put it: “The more info the better.”
The most important insight: “None of the stool tests are incredibly accurate. I use them to fill in pieces of the story.”
This cuts to the heart of diagnostic decision-making in longevity medicine. The best test isn’t the one with the most data, it’s the one that matches your clinical workflow and interpretation style. When tests require confirmatory studies before treatment, you’re adding cost, time, and patient anxiety.
Monday Morning Takeaway:
Choose testing based on your interpretation style: cleaner data for straightforward cases, comprehensive panels when hunting for clues in complex patients. Always use results as one data point in your clinical picture - never standalone. Most panels run $350-500 out-of-pocket. Before ordering, ask: “Will this result change my management?” If the answer is “maybe,” consider treating empirically first.
Secretomes: The Next Frontier or Just Hype
Has anyone heard of secretomes?
The group provided immediate context: secretomes are the growth factors, cytokines, and extracellular vesicles that stem cells secrete to heal tissue ”basically the primordial soup of stem cells.” one doc said.
Then came the critical question: “But if it’s a research product we can’t inject it into people unless as part of a trial?”
The answer was definitive: There are no FDA-approved secretome infusions. Clinical trials are ongoing for heart disease and other conditions, but nothing available for general practice. Timeline to clinical availability: 3-5 years minimum.
This exchange shows how longevity physicians should approach emerging therapies: curiosity tempered by clinical discipline. Secretome therapy sits at the intersection of legitimate science and premature commercialization. The biology is sound: stem cells do work through paracrine signaling. But ‘makes biological sense’ ≠ ‘ready for clinical use.’
Monday Morning Takeaway:
When patients ask about secretome therapy:
Acknowledge: “The science is promising”
Clarify: “It’s investigational: no approved products yet”
Direct: “Check ClinicalTrials.gov for legitimate trials”
Don’t offer it outside approved trials (regulatory risk)
Practice Economics: The NP Compensation Crisis
My NP wants $75/hr for admin time. That’s not sustainable as I don’t get reimbursed.
Thursday’s most engaging thread: “My NP wants $75/hr for admin time—she’s billing 1-2 hours admin for a half-day clinic. That’s not sustainable as I don’t get reimbursed.”
The Market Reality:
Clinical rates: $75-95/hour nationally
Admin rates: Highly variable, same rate to half-rate to capped hours
One physician’s math: “I pay $95/hr for detailed refills and messages, but it definitely adds up.”
Creative solutions emerged: build admin into visit costs but cap ancillary billing, or pay admin at half-rate with monthly hour caps. The brutal truth: “This absolutely kills margin.”
The math reveals a structural problem. If you pay an NP $95 clinical + $95 admin per patient visit ($190 total NP cost), bill $500, factor in 30-40% overhead, you’re at 20-30% net margin before accounting for your time, no-shows, or insurance denials.
Longevity medicine requires more admin time than traditional practice: complex biomarker interpretation, supplement questions, off-label prior authorizations, explaining non-covered services. If you pay the same rate for this as patient-facing time, the model collapses.
Three Compensation Models:
Split-rate: Clinical $85-95/hr, admin 50% of clinical, capped at 50% of clinical hours. Build charting into clinical rate (60-min visit = 75-min pay).
All-in salary: Calculate expected clinical + admin hours monthly. Example: 80 clinical + 40 admin = 120 hours × $85 = $10,200/month. Eliminates hour-tracking disputes.
Concierge pricing: If admin burden kills margins, you’re under-charging. Minimum visit cost = (NP cost + overhead) ÷ 0.6. Below this, you’re subsidizing care.
How to solve it:
If margin pressure is new → Try split-rate model first
If hourly tracking causes conflict → Switch to all-in salary
If neither works → You have a pricing problem (raise rates 30-50%)
Not a member yet? Join the debate in the WhatsApp group
Longevity Docs is a highly vetted, invitation-only community for physicians shaping the future of longevity medicine. Apply to connect with our team.

Each week, I highlight studies that could shape the future of longevity medicine.
This week: AI governance, the best aging clock for mortality prediction
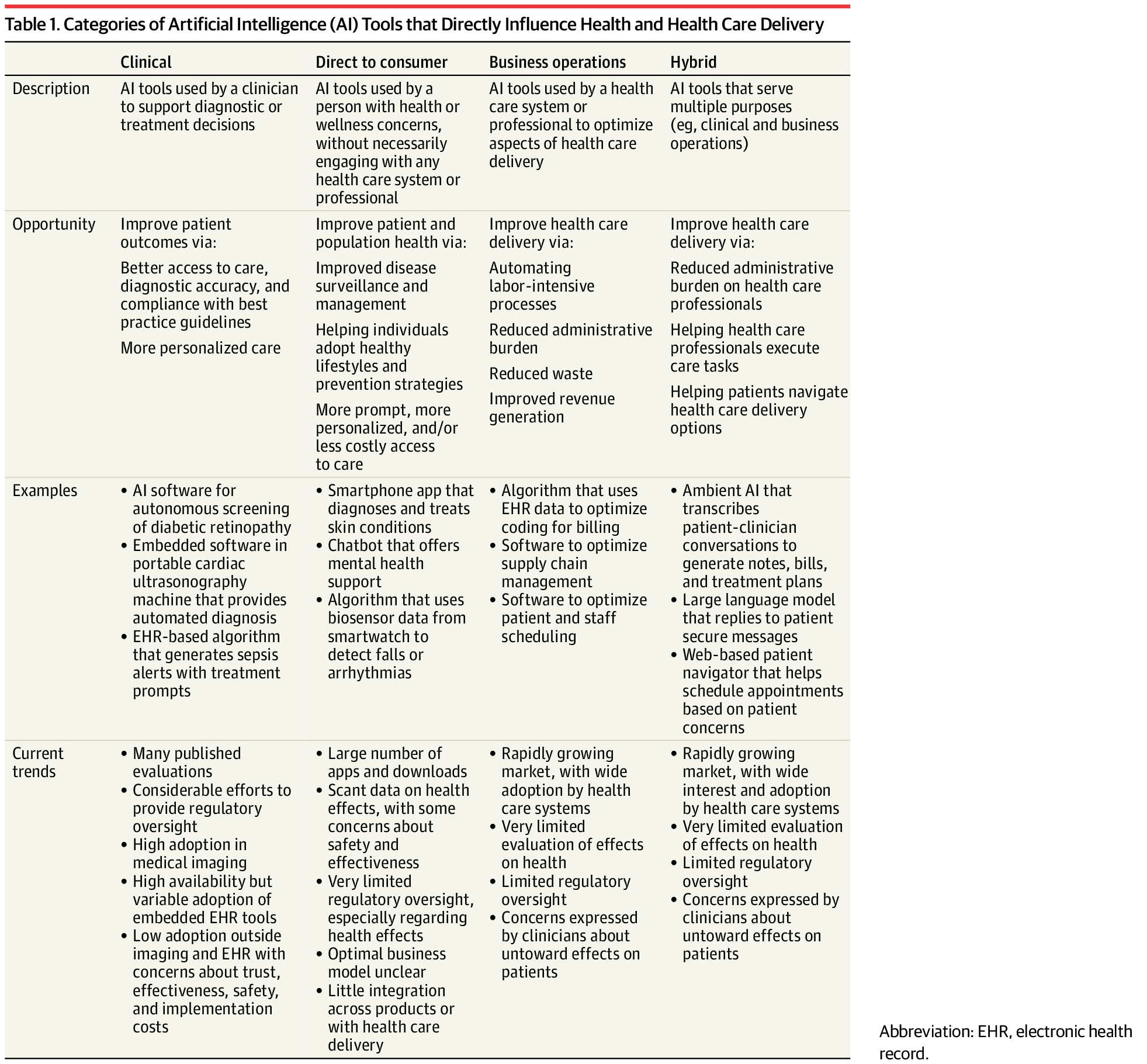
AI in Longevity Medicine: New JAMA Governance Framework
The JAMA AI Summit established guidelines for evaluating healthcare AI tools.
Clinical implication: Demand transparency on training data, require validation in populations matching your patients, and never fully automate clinical decisions.
For longevitydocs: This applies to AI-powered biological age calculators, peptide dosing algorithms, and diagnostic tools entering the market. → Read the full report: JAMA
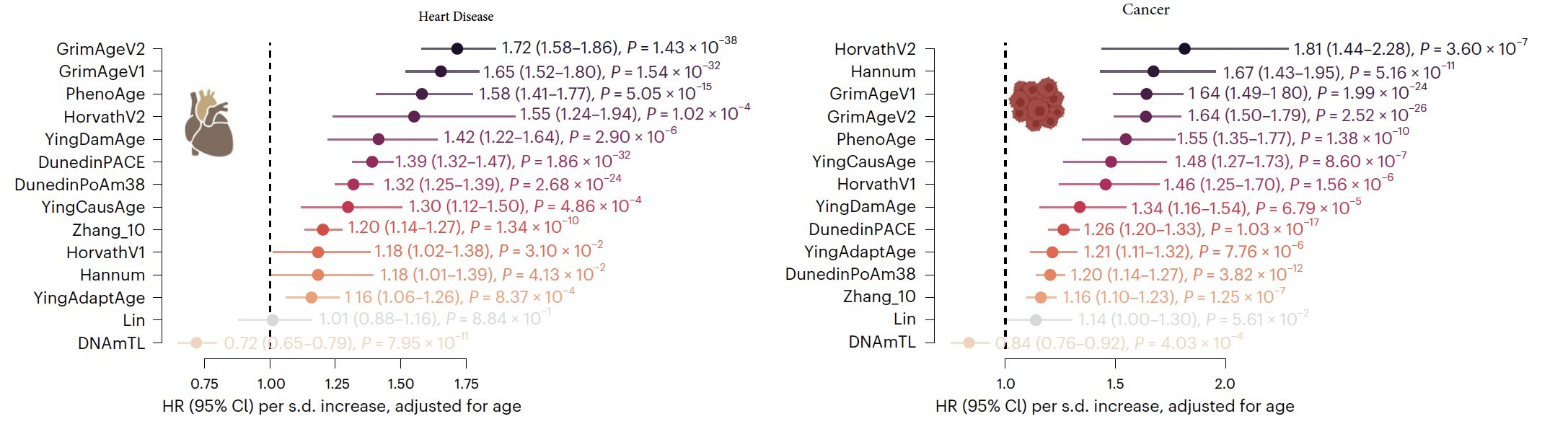
Which Aging Clock Should You Order? New Data
Two major studies this week validate GrimAge2 as the clinical gold standard.
Gladyshev’s analysis of 39 biomarkers across 20,000 individuals shows GrimAge2 has the strongest mortality association. A Lancet meta-analysis confirms higher GrimAge acceleration consistently predicts frailty risk.
For longevitydocs: Current evidence shows GrimAge2 has the strongest associations with both mortality and frailty risk across multiple validation cohorts. Use these findings to interpret DNA methylation results and explain biological age acceleration to patients.→ Nature Aging Lancet Healthy Longevity

Every week, I track funding, FDA approvals, product launches, and breakthrough announcements shaping longevity medicine.
Concierge Longevity Testing Goes Mainstream—and Physicians Must Lead Interpretation
Premium longevity clinics like Biograph ($7,500-$15,000 evaluations) are proliferating, offering whole-body MRI, VO₂ max testing, metabolic panels, and advanced diagnostics. One in six clients uncover serious findings with no symptoms, per Men’s Journal.
For longevitydocs: As screening becomes commoditized, your value shifts from ordering tests to interpreting them. Patients will arrive with pages of data asking “what do I DO?” AI helps parse results, but can’t replace clinical judgment on prioritization and context. Partner with local diagnostic hubs to offer white-glove interpretation services, turning overwhelming data into actionable plans. This is your competitive advantage.
Longevity Becomes National Policy: China’s Billion-Dollar Bet*
The New York Times investigation reveals China’s state-backed longevity push: billions in funding, military hospitals claiming life extension for local leaders, and companies marketing senolytic compounds. Harvard’s Vadim Gladyshev confirms: Chinese researchers “are rapidly catching up” in legitimate science, though “immortality islands” marketing coexists with peer-reviewed research.

The global shift: China isn’t alone. Countries worldwide are positioning longevity as national economic strategy: China’s state investment, Texas’s $3B brain health fund, Saudi Arabia’s biotech initiatives, and emerging European programs signal coordinated government interest in healthy aging.
For longevitydocs: Longevity policy frameworks are being written now at local, national, and international levels. Physicians must engage in these discussions, bringing what policymakers lack: scientific credibility, clinical evidence standards, and expertise measuring both individual health outcomes and population-level impact. Without physician leadership, longevity medicine risks being defined by tech entrepreneurs, supplement marketers, and politicians rather than clinical science. Engage with health policy discussions in your region. Join medical societies shaping longevity standards. Bring clinical evidence to counter marketing hype.
Insilico’s AI Designs 5,000 GLP-1 Peptides in 72 Hours
Insilico Medicine’s Biology42 engine generated 5,000 novel GLP-1 receptor–targeting peptides in 72 hours without referencing known binders. Of 20 synthesized and tested, 14 showed biological activity (70% hit rate), with three achieving single-digit nanomolar potency. AI is compressing years of drug discovery into days.
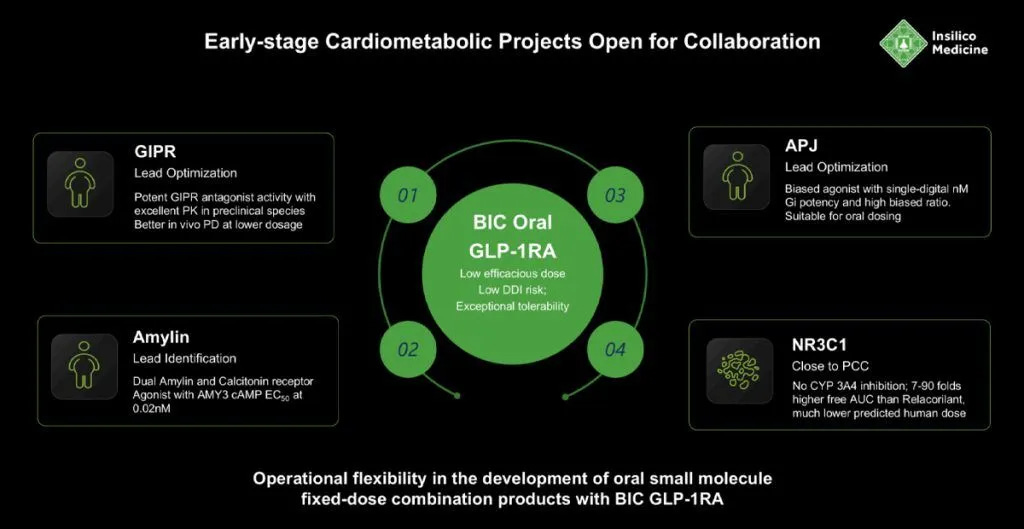
For Longevitydocs: expect a wave of novel GLP-1 variants (oral, longer-acting, fewer side effects) hitting market and trials by 2026. Stay up to date on drug development, because patients expect answers about cutting-edge research, not just traditional care.

Longevity Docs Table: Miami sold out - Boston, LA, SF, Vegas are next

We launched the Table because physicians told us they felt isolated and needed guidance to transform their practice. Each intimate, Jeffersonian-style dinner gathers a curated circle of longevity-minded physicians to share real challenges and breakthroughs, tackling questions no conference can answer.
Miami is sold out. Next cities: Boston, Los Angeles, San Francisco and Las Vegas
Where to Find Us
Miami · Nov 11 - Longevity Docs Table
West Palm Beach · Nov 13 - Eudemonia
Boston · Nov 15 – Harvard Healthcare Conference
Novato · Dec 6-8 – Longevity Clinic Roundtable
Las Vegas · Dec 12-13 – A4M Conference
Palm Beach · Nov 13-16 – Eudemonia Summit
Las Vegas · Jan 6-9, 2026 – CES
New York · January 31 – Longevity Docs AI/Tech Mastermind
Cannes, France · June 9-11, 2026 – Longevity Docs Summit

Longevity Docs is a global education and community platform uniting physicians to make longevity medicine the new standard of care.
With members in 50+ countries, we democratize longevity medicine by giving doctors access to a trusted community, rigorous education, and culture-shaping platforms.
Our mission is to equip physicians with the knowledge, tools, and network to confidently practice evidence-based longevity care. We do this through three pillars:
Community: connecting physicians worldwide into a curated and collaborative network.
Education: providing evidence-based training, certification, and innovation.
Culture: bringing longevity medicine into the scientific and cultural mainstream.
Subscribe to the Longevity Docs Newsletter
Stay connected with a global network of 500+ physicians in 50+ countries advancing longevity medicine. Get evidence-based insights, clinical updates, and exclusive access to the community shaping the future of longevity care.
Newsletter Disclaimer: