

How to Build a $1M Longevity Clinic
#94 Weekly Longevity Medicine Intelligence

Hey Doc,
This one is not for everyone. Most physicians are exceptional at what they do: treating patients in clinical settings, saving lives, practicing medicine at the highest level. That is the backbone of healthcare and it always will be.
But some of you have decided to go a different route. To treat aging before it becomes disease. To extend healthspan by compressing the years we spend living with age-related chronic conditions. Some of you are just starting, either transitioning from another specialty or fresh out of residency. I have been there. I feel you.
Here is what nobody tells you: you need a plan. Not only a clinical plan. A business plan: accounting, legal, marketing, hiring, pricing, operations. None of that is taught in medical school. And yet all of it determines whether your practice survives year one.
Longevity clinics are growing everywhere in the world. There is no going back. But is yours profitable? How do you scale? How do you improve efficiency? I get these questions all the time. There is no perfect playbook, but I want to dedicate this week’s story to the math behind it.
So this week I am writing about how to build a $1M longevity clinic.
11:25am. 94 is out.
Dr. David Luu, Founder, longevitydocs.™

Each week, I try to explore one idea that could advance longevity medicine and hopefully support physicians in bringing it to life.
How to Build a $1M Longevity Clinic?
You are starting you longevity clinic or want to grow it. Like any business, you need a revenue target. I am using $1M because it is the number where investors start paying attention. Whether that means an investment round, or simply building a practice valuable enough to sell when you want to stop (and yes, work is longevity). $1M in revenue is the threshold where your clinic becomes an asset.
These are U.S. numbers. Adapt the math to your market. The models are universal. The price points are local.
And to be clear: we are talking about revenue, not profit. Profit varies based on your cost structure, your geography, your team, and how you run the practice. But you cannot have profit without revenue. So start here.
I get this question all the time. So here are three models, with their trade-offs. I am not including interventions, modalities, or prescriptions here. This is pure longevity care services: membership, testing, consults, coaching. The clinical add-ons are separate revenue lines that change the math significantly depending on your practice.
Three Roads to $1M
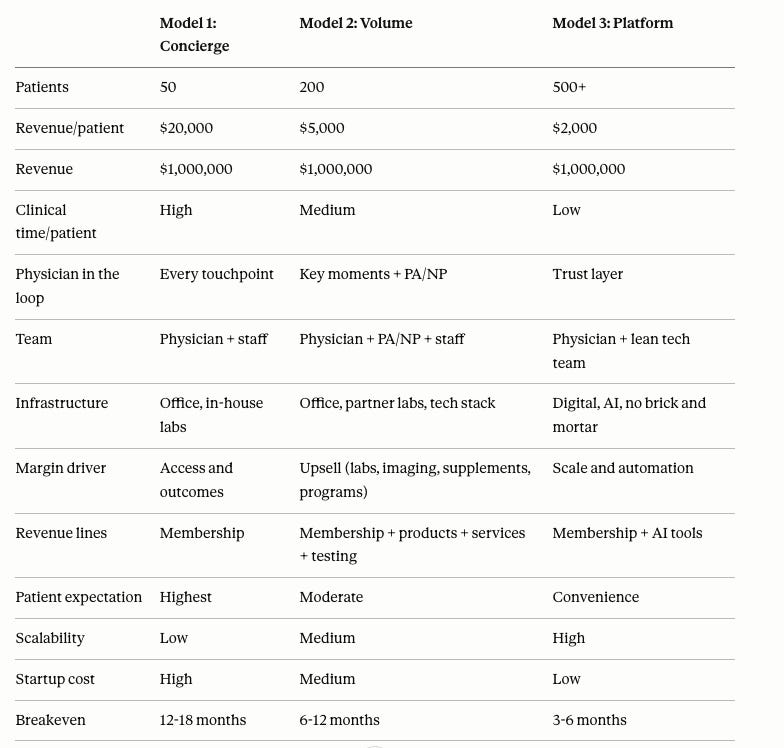
Model 1: Concierge
50 patients. $20K each.
This is the boutique clinic. You see fewer patients, spend more time with each, and charge accordingly.
The math: 50 patients × $20,000 per year = $1,000,000.
Your patients expect full access: your phone, same-day responses, comprehensive testing, personalized protocols. The higher the price, the higher the expectation for outcomes. More human in the loop at every step.
Margins per patient are strong, but your revenue has a ceiling. You are selling your time. At around 50 patients, one physician can deliver. Growth means either raising prices or adding another physician, which changes the business entirely.
Pros: highest revenue per patient, deep relationships, strong retention, simple operations.
Cons: you are the ceiling, burnout risk, small patient base means a few churns hurt, hard to sell the practice without you in it.
Best for: physicians in affluent markets who want a small, high-touch panel and are comfortable being the product.
Model 2: Volume Hybrid
200 patients. $5K each.
Lower entry price, wider funnel. The membership fee covers the clinical relationship, but the clinic does not reach $1M on membership alone.
The math: 200 patients × $5,000 = $1,000,000.
In practice, your $1M usually looks like this: a few hundred thousand from memberships, the rest from labs, imaging, supplements, wellness programs, group consults, and products. Membership gives you the relationship; everything else lives on top of that.
You also need a team. One physician cannot see 200 patients, manage protocols, and run operations. A PA or NP handles follow-ups, routine check-ins, and protocol management. A medical assistant supports in-office testing. A part-time coordinator keeps the calendar and inbox under control.
A real tech stack is mandatory here: scheduling, intake, automated follow-up, patient communication, lab ordering, and data tracking. Without it, this model breaks around 70–80 active patients. Operationally heavier. More moving parts. But at 200 patients with multiple revenue streams, you have a real business.
Pros: diversified revenue, more resilient to churn, buildable team, genuinely sellable business.
Cons: operationally complex, staff management, higher fixed costs, upsell dependency, tech stack is not optional.
Best for: most physician-owners who want a clinic that employs a small team, has an in-person footprint, and is built to be an asset, not just a job.
Model 3: Platform
500+ patients. $2K each.
Digital first. Lightweight physical footprint, if any. AI and automation handle intake, lab structuring, risk scoring, and routine patient communication.
The math: 500 patients × $2,000 = $1,000,000.
In this model, the physician is the trust layer, not the bottleneck. You are not selling your hours. You are selling access to a system with your name, judgment, and protocols behind it. The system does the heavy lifting; you do the thinking.
You review key labs, make decisions, write prescriptions, and coach where it really matters. You can work on an hourly or session-based model and adjust your lifestyle up or down. See patients from anywhere. Work 20 hours a week or 50. Your call.
This is where the physician becomes scalable. The technology makes your brain and your model available to far more people without adding a linear number of hours. This model barely exists at individual-physician scale today, but the economics point here. It has the lowest startup cost, the widest reach, and the highest scalability. It is also the hardest to build, because the technology and regulatory layer have to be right.
Pros: location independent, lifestyle flexible, lowest overhead, highest scalability, highly sellable if built well.
Cons: technology dependency, trust is harder without in-person, relationships are thinner, regulatory complexity across states, the AI layer does not yet exist off the shelf.
Best for: tech-forward physicians willing to build or partner on a platform and expand across regions via telehealth.
The Metrics That Matter (for Every Model)
If you do not know your numbers, you do not have a business. You have an expensive hobby.
Track these monthly:
LTV (lifetime value per patient).
CAC (cost to acquire one patient).
LTV:CAC ratio (you want at least 3:1 or you are buying revenue, not building a business).
Churn (how many members leave per year).
Revenue/margins per physician.
Upsell conversion rate (how many members move into higher-value services).
Lab and testing cost per patient.
Staff cost as a percentage of revenue.
Rent or lease as a percentage of revenue.
Marketing spend as a percentage of revenue.
Tech stack cost per patient.
Breakeven patient count (how many active patients you need to cover your monthly burn).
These numbers tell you which model you are actually running, not which model you think you are running.
The Longevity Clinic Checklist: What You Need Before Patient One
You do not need everything on day one, but you do need a clear sequence. Think in three phases.
1. Before Launch: Non‑negotiables
Legal and Structure
Entity formation (LLC, PLLC, or PC, depending on your state).
Management Services Organization (MSO) with a Management Services Agreement (MSA) if you are separating clinical and business operations.
Business bank account.
Malpractice insurance (confirm longevity/preventive coverage).
HIPAA compliance plan.
Patient consent and waiver templates.
Membership agreement terms.
Accountant (monthly, not just tax season).
Healthcare attorney (one call before launch saves ten later).
Licensing and Credentials
State medical license (and additional states if telehealth).
DEA registration (if prescribing controlled substances).
CLIA waiver or lab partnership agreement.
NPI number.
Collaborative practice agreement (if hiring PA/NP where required).
Core Clinical Infrastructure
Lab partner (or in-house CLIA-waived testing).
Imaging partner (DEXA, CT calcium score, MRI referral pathway).
Pharmacy relationship (including compounding if applicable).
EMR (as your clinical dashboard, not just a billing tool).
Essential Tech and Presence
EMR (there is plenty of them now)
Patient messaging (HIPAA-compliant).
Scheduling (built into EMR or separate).
Payment and membership billing (Stripe, Square, or membership platform).
Telehealth option (HIPAA-compliant).
Simple website: clean, fast, with one clear call to action (book/apply).
2. First 90 Days: Build the Funnel
Team (Part-time is fine)
Front desk / patient coordinator (part-time).
Virtual assistant (scheduling, follow-ups, inbox).
Bookkeeper (weekly).
Marketing and Acquisition
Brand: name, logo, colors, one clear positioning statement.
Website live before you open.
Google Business profile claimed and optimized.
Social media presence (LinkedIn minimum; Instagram if consumer-facing).
Referral network started (PCPs, cardiologists, endocrinologists, therapists).
One lead magnet (free consult, webinar, or guide).
CAC tracking from day one (how much you spend per new patient).
3. Next 12 Months: Scale and Systematize
Advanced Clinical and Data Infrastructure
Wearable data integration (Oura, Whoop, CGM, etc.).
Data aggregation platform for labs and wearables.
Expanded Team (Depends on Model)
PA or NP (essential for Model 2 and Model 3; not required day one for Model 1).
Medical assistant (if you are doing in-office labs or vitals).
Marketing support (freelancer or agency, not full-time yet).
Financial Planning and Review
12-month cash runway or clear revenue plan.
Monthly burn rate calculated before launch and revisited quarterly.
Pricing model locked (membership, per-visit, or hybrid).
Break-even patient count known and updated.
Revenue per patient target set.
LTV and churn assumptions documented and then replaced with real data.
Quarterly P&L review on the calendar.
Where AI Fits
AI coaching on labs will become a commodity. Every report will start to sound the same. That is fine. Let the machines summarize.
What remains scarce is the physician: your trust, your guidance, your judgment, your ability to motivate and hold patients accountable. That layer is not going away in three years. Probably not in ten.
Build your clinic so that AI and software handle everything repeatable—and you focus on the work that only you can do.
Choose Your Model, Know Your Math
Pick the model that matches your risk tolerance, your lifestyle goals, and your market:
Boutique (50 × 20K).
Volume hybrid (200 × 5K).
Platform (500 × 2K).
And if $1M feels far away, remember: Model 2 is 200 patients at $5K. That is 17 new patients a month for a year. One physician, one PA, one tech stack, one year.
The time to build is now. We will go deeper into these models in at the Longevity Docs Summit in Cannes in few weeks.

Every week, the Longevity Docs Chat feels like a front-row seat to the future of medicine. Here’s what had doctors buzzing:
Is there a clinical difference between tirzepatide and semaglutide for reducing alcohol cravings and tolerance?
A physician who prescribes both shared his experience: tirzepatide is more effective for cravings specifically, but semaglutide also works well for reducing overall intake. AUDIT score reductions are comparable in his clinic.
Another member added a practical observation: patients eat less on both medications, which means they hit higher blood alcohol levels faster when they do drink. “They end up pregaming harder than they used to party.”
A third member asked whether the effect differs between branded formulations (Mounjaro vs Zepbound vs semaglutide). The consensus: the molecule matters more than the brand. Tirzepatide’s dual GIP/GLP-1 mechanism may explain the stronger craving reduction, though head-to-head data in alcohol use disorder does not yet exist.
Separately, a member flagged two GLP-1 drug interactions from recent literature: risk of hypercalcemia when combined with thiazide diuretics or calcium supplements, and increased lithium levels in patients on lithium therapy.
Key Takeaways: tirzepatide may have an edge over semaglutide for alcohol cravings, but both reduce intake. Monitor patients who drink on GLP-1s for faster intoxication due to reduced food intake. Check for thiazide and lithium interactions. Head-to-head data is needed.

PCOS Is Now PMOS
Polycystic Ovary Syndrome is officially renamed Polyendocrine Metabolic Ovarian Syndrome (PMOS). The Endocrine Society and more than 50 global patient and professional organizations led the change after 14 years of collaboration. The old name reduced a complex, long-term hormonal disorder to a misunderstanding about ovarian cysts. There is actually no increase in abnormal cysts on the ovary. PMOS affects 1 in 8 women worldwide, more than 170 million. The new name leads with hormones and metabolism, reflecting what the condition actually is: a multi-system endocrine disorder with impacts on weight, metabolic health, mental health, skin, and the reproductive system. A three-year transition period begins now, with full implementation in the 2028 international guideline update. Endocrine Society
Why it matters: the name was a barrier to diagnosis and care for decades. Physicians and patients both defaulted to thinking “ovarian cysts” when the real drivers are hormonal and metabolic. For longevity physicians treating women’s health, this reframe aligns PMOS with the metabolic and endocrine lens already used in practice. Update your clinical language now. The guidelines will follow.
Sleep Duration and Biological Aging: The U-Shaped Curve Across Every Organ

A new Nature study of nearly 500,000 UK Biobank participants mapped sleep duration against 23 biological aging clocks across organs and omics layers. The pattern is U-shaped everywhere. Both short (under 6 hours) and long (over 8 hours) sleep accelerate aging in the brain, liver, lung, immune, endocrine, and adipose systems. The sweet spot: 6.4 to 7.8 hours. Both extremes raise all-cause mortality (HR 1.4 to 1.5), but through different routes. Short sleep acts directly on systemic disease risk. Long sleep appears to be a signal of underlying organ aging already in progress.
Why it matters: Sleep duration is a cheap, modifiable vital sign that tracks biological age across the whole body. Seven hours is not a lifestyle recommendation. It is a biomarker. Ask about it at every longevity visit.
Beta-Blockers May Protect Against Vascular Dementia. ACE Inhibitors May Not.
Researchers used Mendelian randomization across 46 drug targets and nearly 900,000 controls to test whether existing lipid-lowering, antihypertensive, and anti-inflammatory drugs could be repurposed to prevent vascular dementia. Beta-blockers targeting the ADRB1 receptor showed the strongest protective signal. ACE inhibitors showed the opposite: a potential increase in vascular dementia risk. Most other drug classes showed no effect. Nature Aging
Why it matters: vascular dementia is the second most common form of dementia and shares biology with cardiovascular disease. Many longevity patients are on antihypertensives. If beta-blockers protect the brain while ACE inhibitors do not, that changes how physicians weigh cardiovascular and cognitive risk together. For patients on ACE inhibitors, this is worth watching as pharmacovigilance data catches up.

Every week, I track funding, FDA approvals, product launches, and breakthrough announcements shaping longevity medicine.
AI / TECH
Doximity Launches Free Prescribing for Physicians
Doximity released Doximity Prescribe, a free prescribing tool built into the platform through a partnership with Photon. Physicians write the prescription inside Doximity. The patient receives a text to choose their pharmacy and view estimated costs before pickup. No extra portals, no pharmacy calls. Fully mobile. Free for all verified U.S. physicians, NPs, and PAs. For longevity physicians running cash-pay practices, patients seeing costs upfront and choosing their own pharmacy removes the friction that eats clinical time. Doximity
Function Health Acquires SuppCo. The Supplement Trust Problem Gets a Data Layer.

Function Health acquired SuppCo, a supplement verification platform that has rated 35,000+ products and analyzed 500,000+ routines. SuppCo’s independent testing found roughly half of top-selling supplements failed basic label accuracy. Function plans to connect supplement data to its existing biomarker platform so patients can see whether what they take actually moves their numbers. No supplement sales, just scoring and verification. For longevity physicians, this is the infrastructure that turns “should I take this?” from an opinion into a lab-verified answer. Longevity Technology
POLICIES
Makary Out at FDA. What It Means for Longevity Therapeutics.

Marty Makary resigned as FDA Commissioner on May 12. His replacement, acting commissioner Kyle Diamantas, is a food-industry lawyer with no medical or scientific background. Makary was polarizing, but he lowered the bar for drug approvals in ways that mattered for aging science: single pivotal trials instead of two, and a plausible mechanism pathway for rare disease drugs. Senolytics, rapamycin analogs, NAD precursors don’t fit traditional approval frameworks. Makary’s FDA was at least asking the question. Physicians should watch whether those pathways survive the transition or get quietly shelved. STAT News
SCIENCE
900 “Dark Proteins” Mapped Across 32 Cancers. Proteomics Is Moving Faster Than Genomics.

Researchers mapped roughly 900 "dark proteins," proteins with no known function, across 32 cancer types using mass spectrometry on more than 1,100 tumor samples. Several of these dark proteins sit on cell surfaces, making them viable targets for immunotherapy. One candidate, C1orf116, showed up consistently in head and neck squamous cell carcinoma and is now being tested as a CAR-T target. The study reframes the proteome: the proteins we have ignored may matter more than the ones we have studied. For longevity physicians tracking cancer risk as part of biological aging panels, this is a signal that protein-level diagnostics are moving faster than genomics alone. STAT News

Discover who is going Back to Medicine
Longevitydocs Cannes Summit & Awards- June 9-11








































The Home of Longevity Medicine
longevitydocs.™ is the world’s leading longevity physician community - 1,000+ physicians across 68 countries united by a single conviction: every doctor should be a longevity doctor. Founded by Dr. David Luu, the platform offers its members network, education, and experience with the mission to democratize longevity medicine.
Not a member yet? Join longevitydocs™
We’re a physician-only network. Curated. Vetted. Built on trust. If you’re committed to practicing longevity medicine with rigor, peer support, and shared standards → this is your community. Apply to connect with our team.
Longevity medicine is the personalized, evidence-based practice of modifying the root mechanisms of aging (biological, cognitive, and psychosocial) before they become disease, extending healthspan, not just lifespan. Using advanced diagnostics, precision interventions, and AI-enabled monitoring, it translates measurement into action across every medical discipline. Success is measured in functional capacity, vitality, and disease-free years.

Subscribe to the Longevity Docs Newsletter
Longevity medicine is moving fast. Every week, we bring you what matters: clinical insights, research signals, and perspectives from 1,000+ physicians across 68 countries. One newsletter. Built for the physicians shaping this field.
Editorial Disclaimer:
Too late. Environment keeps us unwell. 2050 to 3000 MAYBE climate will improve...only then can we focus on healthspan. Not promising.
This was an excellent read! Thank you David! I am going to keep referencing this as I continue to grow my business in longevity primary care 💪💪