

Hormones Mastermind NYC • Plaque Reversal Breakthroughs • Gen AI in Aging Science
Your sneak peek into the world of Longevity Docs.

Hey Docs,
Greetings from Davos, where longevity and AI are taking center stage. It’s energizing to see how much attention is being given to key challenges like longevity education and the critical bottleneck of training healthcare professionals in longevity medicine.
On that note, I’m thrilled to announce the Longevity Docs Hormones Mastermind, happening on March 29th, 2025 in New York City. This physician-only event will feature top hormonal health faculty and a curriculum designed to elevate your practice with evidence-based strategies in hormonal health and longevity.
Happy Sunday!
Dr. David Luu
🧬 Community
The Hormones Mastermind will take place in NYC on March 29th, 2025
We heard you loud and clear: deeper, focused education on key topics. That’s why we’re thrilled to announce our first curriculum on Hormonal Health and Longevity
📅 Date: March 29th, 2025
📍 Location: NYC (In-person & Digital Access Available)
This one-day, 10-course curriculum features dozen world-renowned experts, offering an unique opportunity to elevate your expertise in hormonal health and longevity medicine.









Meet the World-Class Faculty
Learn directly from an unparalleled lineup of physicians, including:
Drs. Amy Killen, Jessica Shepherd, Elizabeth Yurth, Angela DeRosa, Salome Masghati, Juan Bautista, Felice Gersh, Melissa Loseke, Marcos de Andrade, Elizabeth Poynor, Kyle Gillett.
Curriculum Courses
Foundations of Hormonal Health for Clinical Practice
Identifying Patients for Hormone Therapy
Diagnostics & Biomarker Interpretation for HRT
Designing Safe & Effective Hormone Protocols
Clinical Benefits of Hormone Therapy: What to Expect
Managing Risks & Side Effects of Hormone Therapy
Integrating Cutting-Edge Therapies into Your Practice
Non-Hormonal Adjuncts to Optimize Hormonal Health
Navigating Regulatory Requirements & Best Practices for Prescribers
Establishing a Successful Hormone Therapy Practice
Seats are limited to ensure maximum interaction and value. Don’t miss your chance to be part of this exclusive event.
This is your opportunity to connect, learn, and lead. Will you be there?
Longevity Docs Hormones Mastermind | March 29th, 2025 | NYC
💬 Buzz in the Chat
Im trying to create a reasonable “neurocognitive prevention screen” for my patients interested in being proactive.
So far Im considering:
Labs:
Apo E4 testing
P-Tau 181
P-Tau 217
Amyloid AB42 / AB 40 ratio
Imaging:
Carotid ultrasound
+\- MRI brain.
Administered testing: +\- Creyos +\- WAVI.
Anything else specific to neurocognitive testing people like to use or think I should take out? Any advice would be appreciated 🙏
Add nfl, GFAP, and TGF-b1
I’d like to expose a scenario to you all in regards to PLAQUE.
Doc 1: Re: cleerly exams and evolution and PCSK-9 inhibitors and other agents that can slow down progression.
So I will add here an image of a before and after of a cleerly heart exam that 10 months later is significantly worse as it relates to a specific vessel (RCA) had zero stenosis and 10 months later jumped up to a whopping 21% stenosis. However the overall calcified plaque went down (not normal). So soft plaque went up considerably and calcified plaque went down. This patient did start using repatha about 25 days before the second cleerly exam so I am hoping this is due to plaque remodeling.
we are seeing this interplay of cleerly exams more and more and now with the different PCSK-9 inhibitors, I’m wondering if someone here has seen better reversal or plaque stabilization with for example inclisiran vs repatha.
Lipoprotein a hovers between 20-32
APOb hovers 110-130
Just have always had a lot of LDL small 300-650
And crazy healthy guy and very fit.
We are doing more and more cleerlys and we are seeing ppl build up more plaque than we thought. The cleerly report is always worse than the CTA and calcium score. So then the question is do we start medicating these ppl and what do you all find works best results on the cleerly. I have even read that colchicine and repatha offer good results. Also I am reading more on plaquex (phosphatidylcholine). Seems promising.
Doc 2: RCA is the vessel that is most prone to artifact on CT angio. This is a possibility. Consider having an experienced cardiac imaging specialist review both studies.
Cleerly has a comparison tool on their portal that will allow more in depth analysis of the differences. This tool creates a detailed summary table of the differences between exams.
1 cubic millimeter of change in calcified plaque is within the error of the test - not a significant difference.
Assume that ApoB is pre Repatha. I’ve never seen one that high on the drug.
Doc 3: I have to admit this pushes me back into concern regarding CLEERLY
Radiation exposure. Dye exposure. No robust randomized control trials showing superiority regarding mortality vs a number of other possible ways to manage risk that are either very low, or even no radiation (for instance lower extremity Doppler studies combined with carotid plaque quantification or CIMT and Coronary Calcium Score.
The supposed accuracy of CLEERLY, which I I’m not doubting still may be the case with you - or anyone checked within recent window of PCKS9 initiation – as an outlier. But we are not chasing images. We need to chase real morbidity and mortality events with things like imaging being interesting, but not ready for prime time to start adding concern, risks, exposure to cost and potential side effects of medication‘s (though I’m a big proponent of PCKS9 inhibitors so far).
I’d be willing to bet that your lack of family history, parents who have imaging that looks great (and presumably no better lifestyle than you have had), despite being older (and I bet you have great blood pressure too but that should be clarified) with no personal smoking history, Active… I’m sorry but I would leave it at the PCKS9 if you can afford it and continue to keep your blood pressure, lipids and insulin sensitivity under control and live and enjoy your life. Longevity interventions that reduce quality of life, inject anxiety and are not Robustly proven or, to me, one of the main issues that can keep us from legitimacy as a movement that should be as reasonably evidence based as possible.
In your case the odds of “much ado about nothing“ or maybe a (“making mountain out of a) molehill” are fairly high from what I gather. So it’s not always that when it “walks like a duck” 🦆 and “quacks like a duck” 🦆, that we end up needing the autopsy of the duck.
No I guess one thing I could ask is by “crazy Healthy” does this include extreme exercise? Because of course extreme exercise has been associated with accelerated calcification of the coronary arteries and, while impressive and certainly maybe a legitimate calculated lifestyle risk, shouldn’t be perceived as done for longevity.
Now this is just one guy’s opinion in this group and you can take it or leave it and I’m not expecting anyone else, or many, to agree but I would still feel confident in my perspective and hope that it’s added some food for thought.
🩺 Publications
Deep learning and generative artificial intelligence in aging research and healthy longevity medicine
This review examines how Deep Learning (DL) and Generative Artificial Intelligence (GenAI) are used in biomarker discovery, deep aging clock development, geroprotector identification and generation of dual-purpose therapeutics targeting aging and disease.
Aging - Recommended by Dr. Tom Rifai

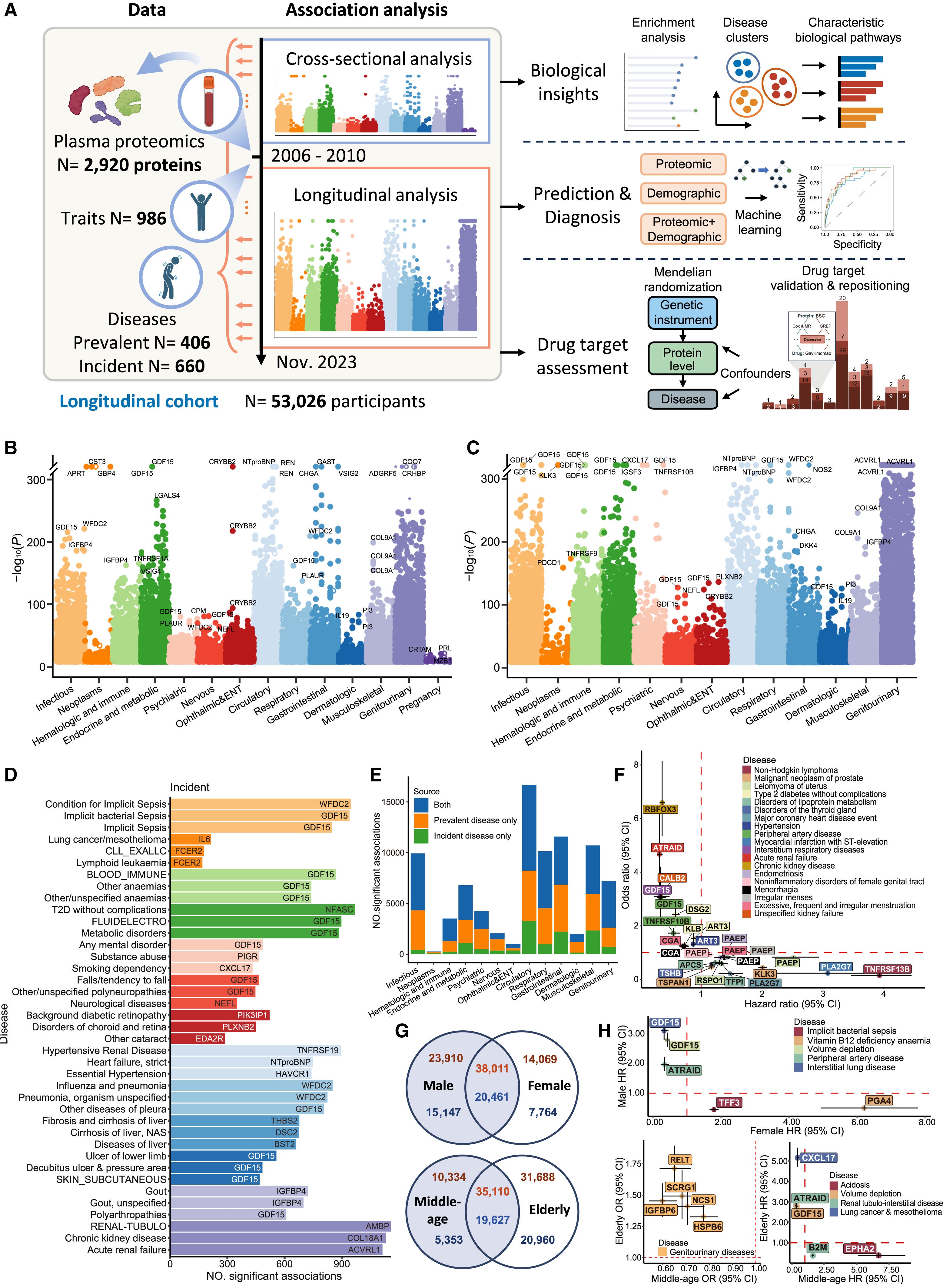
Atlas of the plasma proteome in health and disease in 53,026 adults
Open-access comprehensive proteome-phenome resource to help elucidate the biological mechanisms of diseases and accelerate the development of disease biomarkers, prediction models, and therapeutic targets.
Cell - Recommended by Dr. David Luu
New American Heart Association Scientific Statement on Lipoprotein Apheresis
With a single session, LA reduces Lp(a) and LDL-C levels by 65% to 85%; reduces inflammatory markers, prothrombotic factors, atherogenic HDL-C components, blood viscosity, and endothelial dysfunction; and improves microvascular myocardial perfusion, suggesting multiple potential mechanisms by which LA may modulate ASCVD risk.
AHA Journal - Recommended by Dr. Darshan Shah
🌐 In the Media
Longevity Breakthrough: Scientists Restore “Youthful” Enzyme Activity To Combat Aging
Too old for healthy aging? Exploring age limits of longevity treatments
🗓️ Upcoming Events
Longevity Investors Lunch - Davos, January 21, 2025
Founders Longevity Forum - Singapore, February 27-28, 2025
Longevity Docs Hormones Mastermind - NYC, March 29, 2025
Vitalist Bay - Berkely, CA, Apr 4 - May 29, 2025
The Longevity Med Summit - Lisbon, May 6-8, 2025
Life Summit - Berlin, May 27-28, 2025
Longevity Docs Cannes - Cannes, Juen 25-26, 2025
🚀 5 Reasons to Join Longevity Docs
Join a Trusted Network of Leaders
Become part of a highly-vetted community of over 250 longevity physicians spanning 40 countries, committed to advancing evidence-based longevity medicine.Access Unparalleled Events and Insights
Attend one-of-a-kind events like the Cannes Longevity Docs Festival, New York Masterminds, and retreats. These gatherings bring together the brightest minds shaping the future of longevity medicine.Lead the Way in Research and Innovation
Contribute to real-world evidence research, clinical trials, and patient registries. Be among the first to implement the breakthroughs transforming healthcare and longevity practices.Elevate Your Practice and Knowledge
Gain insider access to cutting-edge protocols, masterclasses, and clinical resources that help grow your practice and enhance your impact on patients’ lives.Shape the Future of Longevity Medicine
Collaborate with peers to build the future of healthcare, making longevity medicine more effective, accessible, and impactful for patients worldwide.
⚡ Join Now: Together, We’re Redefining Medicine. Be part of a global network making a difference—apply today!
Newsletter Disclaimer:
The content shared in this newsletter, including the "Buzz in the Chat" section, is for educational purposes only. It is derived from peer-to-peer conversations among physicians within the Longevity Docs community and is intended to inform and engage our network of doctors.
Please note that these discussions do not reflect the official position of Longevity Docs and are not to be interpreted as medical advice or recommendations. The insights and opinions shared are those of individual physicians and are provided as part of our mission to foster collaborative learning and dialogue among healthcare professionals.
We encourage all readers to consult qualified healthcare professionals for personalized medical advice and to evaluate any medical information in the context of their clinical expertise and patient needs.
Subscribe to the Longevity Docs Newsletter
Stay connected with the backstage of the Longevity Docs community, a network of over 250 physicians spanning 40 countries, united in our mission to democratize longevity medicine. Explore the latest in evidence-based longevity care, gain exclusive access to physician insights, and join us in shaping the future of this transformative field.
Who’s speaking?