

Are Peptides The New Cannabis?
#90 Weekly Longevity Medicine Intelligence

Hey Doc,
It is 5:07am. New York City is dark. Like every Sunday, I start the newsletter from a blank screen, coffee in hand, the city not yet awake. I love this moment.
This week’s conversations were about peptides and platforms. Regulations, risks, science, media. The pattern reminded me of the cannabis era, so I went deep into the history, the correlations, the question of whether history repeats itself.
I asked myself: are peptides the new cannabis? Will peptide shops sit on the same sidewalks of SoHo, next to our favorite yoga studio?
Still committed to the mission: making longevity medicine the new standard of care. Every doctor should be a longevity doctor.
This is Newsletter 90. The unfiltered, unsponsored version of my reflections on longevity medicine.
Dr. David Luu - Founder, longevitydocs.™
PS: Are you getting ready for Cannes? Email me back here. I read every message. I reply to everyone.

Every Wednesday, we ship something new for this community. Features, experiences, and products built by physicians, for physicians. The platform grows because you do.
We are launching Events
Peer learning has always been a medical tradition. The conference was just the easiest format.
There is no community without programming. A once-a-year gathering is not enough.
We started with a chat. Then online masterclasses. Our first in-person mastermind. The Summit and Awards in Cannes. Roundtables in different cities. Now Rooms.
Each one built for physicians, by physicians.
The new Events feature on the platform brings it all under one roof: our programming, and the events of partners we trust.
A year-round commitment to the kind of learning that actually changes how we practice longevity medicine. We build what doctors will use to take better care of their patients.
ROOM
What Happened in the Room stays in the Room
but we’d like to share the key takeaways
Last Wednesday we launched Room: live, 20-minute peer sessions on longevitydocs.ai. Here’s what physicians took home.
Room 1: How to Practice Longevity Medicine - Dr. David Luu + guest Dr Steven Murphy
Add a longevity layer to your specialty. If you are a cardiologist, go deeper into cardiovascular aging, prevention, data, wearables, and emerging therapies. Build on the expertise you already have. That is the fastest path to outcomes.
Pick one niche to serve everyone. Trying to serve everyone dilutes the offer. Choose one audience, go deep, and build the practice around them. Depth creates referrals, reputation, and pricing power. Fit matters on both sides: not every patient belongs in your practice, and not every physician is right for every patient. Be intentional about who you take on. The wrong fit drains the team. The right fit compounds trust over years.
Serve patients like five-star hotel guests. Every touchpoint, from first inquiry to follow-up, should signal the same level of care as the clinical work. Loyal patients are your best marketing. Invest in the experience and the practice compounds on its own.
Do not over-invest in shiny technology you cannot leverage. Outsource it. Partner with specialists who own the tech layer so your attention stays on clinical work, strategy, and relationships. Tools should serve the practice, not distract from it.
Build a Formula One team. Longevity medicine is a team sport. Surround yourself with operators, clinicians, and support staff who execute at the highest level. The physician stays in the driver’s seat on clinical judgment and strategy. Everyone else makes the car faster.

Room 2: Gut Health Reset - Dr. Mishal Reja
Treat IBD as a systemic inflammatory disease, not a gut condition. The gut is the central hub of the immune system, wired directly to the vagus nerve, with downstream effects on neurological health, skin, mood, weight, and oncogenesis. Approach it as a longevity lever, not a GI problem.
Work the triple pathophysiology stack. Genetics set the stage. Environment pulls the trigger: emulsifiers, glyphosate, early-life antibiotics, and microplastics now documented in UC and Crohn’s tissue. Stress drives it through cortisol’s mucolytic action on the mucus layer. Miss any axis and you miss the disease.
Run a longevity-grade workup across all three axes. Pair standard labs and SIBO testing with inflammatory gut markers, genetic panels covering oxidative stress and detox pathways, and total toxic burden testing for mold, metals, and environmental exposures. Only order tests you can act on.

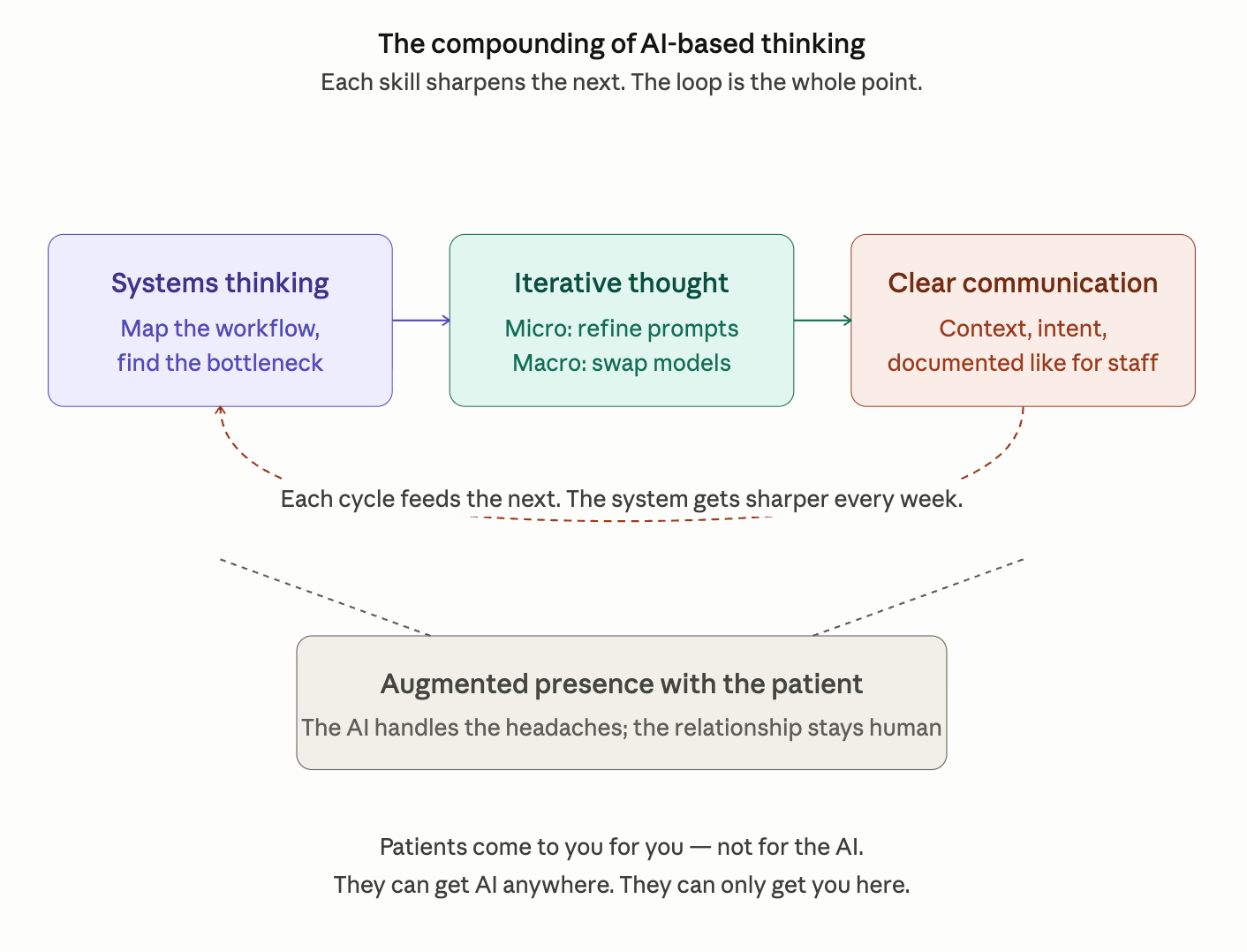
Room 3: The AI Tech Stack for Your Practice - Dr. Omar Saleem
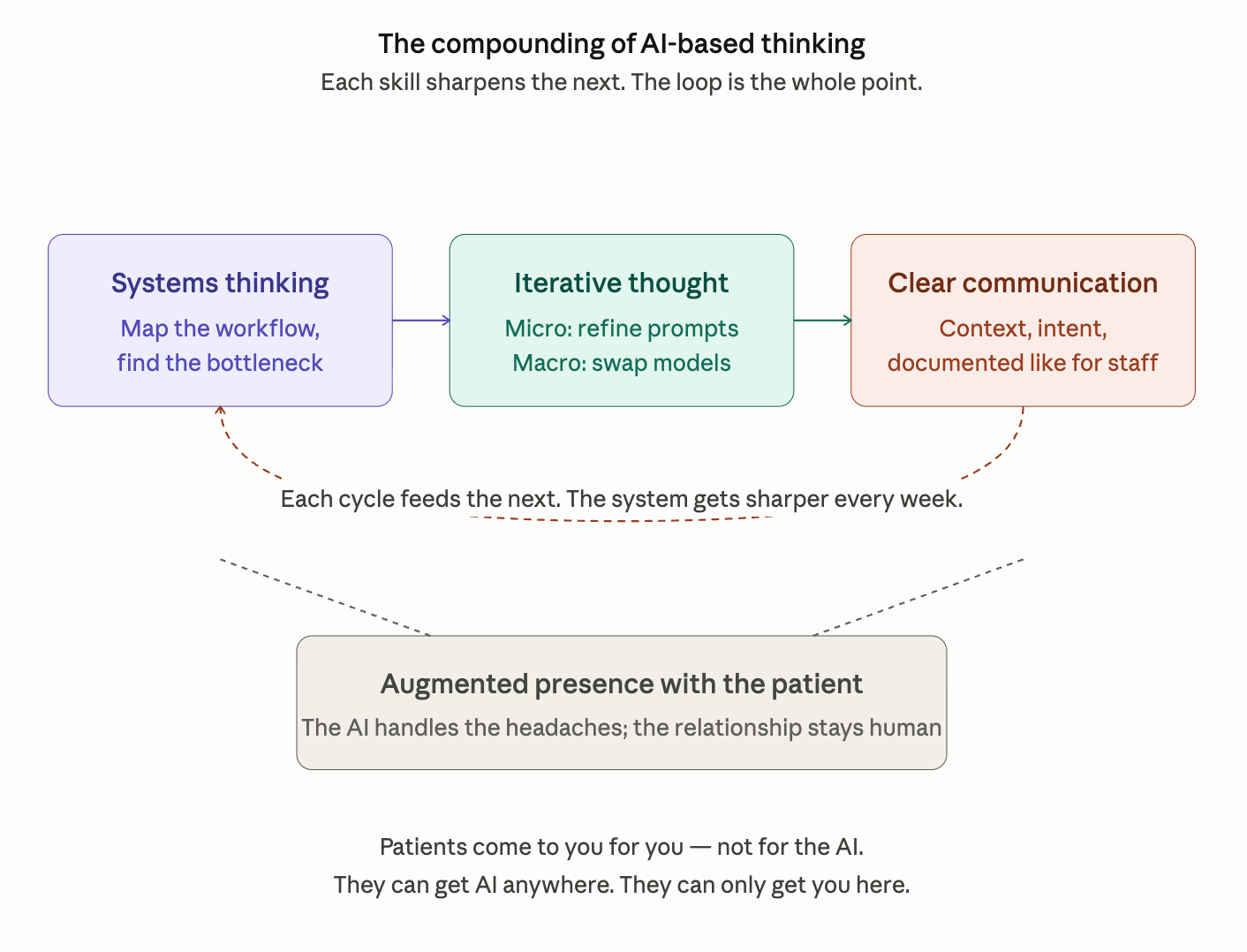
Start and go deep on two or three tools, not twenty. Tool minimalism beats tool maximalism. A workspace suite, a general-purpose LLM, and a second-brain note system is enough to run a modern longevity practice. Chasing every release is a tax on attention.
Think in systems, not tools. Design an ecosystem, iterate at both the prompt level and the practice-design level, and communicate with precision. AI’s real strengths are synthesis and coordination. Both depend on clarity of instruction.
Respect the HIPAA/GDPR split. It is the non-negotiable design constraint. Workspace suites with a signed BAA are compliant for patient data. Most consumer LLMs are not. Operating rule: general LLMs for everything non-clinical, BAA-covered tools exclusively for patient data.
Invest in trust, not tech. As building commoditizes, trust is the final product. A usable longevity practice site is now a prompt away. AEO is overtaking SEO, with the bulk of traffic flowing through one dominant LLM. What stays defensible is domain expertise and patient relationships. Let AI handle admin so you spend more time on the relationship.
Automate your Monday-morning prep. It is the highest-leverage AI use case in the practice. An agent workflow that reads the day’s schedule, pulls each patient’s labs from storage, and produces clinical briefings can collapse hours of prep into under 30 minutes. Treat clinical decision support as a watchful second tier where emerging longevity literature still requires source verification.
Next Rooms
This week's full programming is live on the app. Don't miss the live conversations.



Each week, I try to explore one idea that could advance longevity medicine and hopefully support physicians in bringing it to life.
Are Peptides the New Cannabis?
A personal reflection for physicians. Science evolves. Regulation evolves. Our professional obligation does not: protect patients and practice within the law using the best evidence available at the time.
Recent announcements about peptide reclassification made me think of the cannabis story. So I went down a rabbit hole this morning.
I see patterns worth a moment of reflection.
Here is what I saw and what I think it means for how we educate and empower ourselves as a community.
The cannabis story, briefly
Cannabis did not begin as a counterculture product. It entered Western medicine in the nineteenth century, appeared in the U.S. Pharmacopeia by 1850, and was prescribed through normal pharmacy channels for decades.
Then policy shifted. The Marihuana Tax Act of 1937 restricted medical access. The Controlled Substances Act of 1970 placed cannabis in Schedule I, blocking most research and routine prescribing. Demand did not disappear. It just became illegal. Clinicians stepped back. State-level reforms began reopening medical access with California in 1996.
The pattern: Discovery → Adoption → Restriction → Gray market → Incremental legitimization → Commercial scale.
The peptide story, so far
The peptide story starts with insulin in 1921. A century later, dozens of FDA-approved peptide drugs sit firmly in mainstream practice.
Then came GLP-1s.
Exenatide was approved in 2005. Liraglutide in 2010. Semaglutide in 2017. What began as a diabetes medication became, by the early 2020s, one of the fastest-adopted drug classes in modern medicine — reshaping how healthcare systems, payers, and patients think about metabolic disease, obesity, and preventive care. The GLP-1 class alone is now a market measured in the tens of billions, with manufacturing capacity still racing to catch up with demand.
That is the visible, regulated track. Discovery, decades of development, large trials, approval, and scale.
A second track developed more quietly. Over two decades, 503A compounding pharmacies and clinicians used compounded peptides — BPC-157, CJC-1295, Ipamorelin, thymosin alpha-1, TB-500, and others — where mechanistic rationale was plausible and bedside experience was ahead of large-scale trials.
In 2023, the FDA moved a group of peptides to Category 2 of the 503A bulks list, ending their eligibility for standard compounding. In 2024, PCAC declined to recommend adding several peptides to the approved list, citing limited U.S. outcomes data. In 2026, FDA signaled reconsideration of approximately a dozen substances, with meetings scheduled in July 2026 and February 2027.
The outline: Discovery → Adoption → Restriction → Gray/alternative channels → Potential reconsideration.
The story is still being written and GLP-1s are a reminder that when a peptide class does cross the full regulatory arc, the impact on medicine can be generational.
The Comparison Between the Cannabis and Peptide Stories

The two stories trace the same shape. A scientific breakthrough. Decades of legitimate pharmacy use. A restriction event that redirects demand rather than eliminating it. Physicians practicing between observation and evolving regulation. A slow, uneven path toward reconsideration.
The differences matter too and they are worth naming carefully.
What this means for the physicians community
This is where I think the pattern is useful.
Peptides, like cannabis, are one chapter in a longer story of emerging modalities. Others will follow. What does not change is our obligation as physicians. What can change, and what this community is built to change, is how prepared we are when the next chapter arrives.
Four things each of us can do, independent of where the regulation lands.
Educate. Stay fluent in the evidence, the mechanisms, and the regulatory framework that governs our practice. Emerging modalities reward physicians who understand the science before the marketing. Longevity Docs exists to make that education continuous, peer-reviewed, and physician-led.
Stay updated. Regulatory landscapes shift. FDA, PCAC, state boards, and international bodies move on their own timelines. A community that tracks these changes in real time (and translates them into clinical language) protects every physician in it.
Run research. Advisory committees declined several peptides in part because organized U.S. outcomes data was missing. That is a gap a physician community can close. Clinician-led registries, standardized data capture, and shared protocols turn individual bedside experience into evidence the next regulatory cycle can actually weigh.
Operate legally and ethically. Stay within the boundaries of current law. Careful patient selection. Informed consent. Transparent communication about what is known, what is unknown, and what may change. Documentation that holds up to scrutiny. This is the posture that outlasts any regulatory cycle.

Every week, the Longevity Docs Chat feels like a front-row seat to the future of medicine. Here’s what had doctors buzzing:
Does mTOR Inhibition increase Lipids?
A clinical thread emerged around rising LDL and triglycerides in patients on mTOR inhibitors and whether the community is measuring the wrong things.
One physician laid out the mechanism clearly:
“mTOR2 inhibition drives the hepatic insulin pathway toward higher TG and LDL. Another possibility is increased breakdown of adipose, which means more FFAs delivered to the liver which then converts FFAs to TGs.”
He kept going, reframing it as a feature, not a bug:
“If we are pushing metabolism more towards autophagy and energy conservation you can see higher circulating cholesterol. Fat is being mobilized, not stored.”
Then the sharp critique:
“They should have checked ApoB and they missed the mark there. I wouldn’t be surprised if there was elevated LDL but no major increase in ApoB. They should also monitor fasted insulin.”
Key takeaway for Longevitydocs:
If you’re dosing rapamycin or any mTOR-targeting protocol and tracking standard lipid panels, you’re reading the wrong instrument. LDL elevation under mTOR inhibition could reflect fat mobilization and autophagy. ApoB and fasted insulin could be a better signal.

Public use of a generalist LLM chatbot for health queries
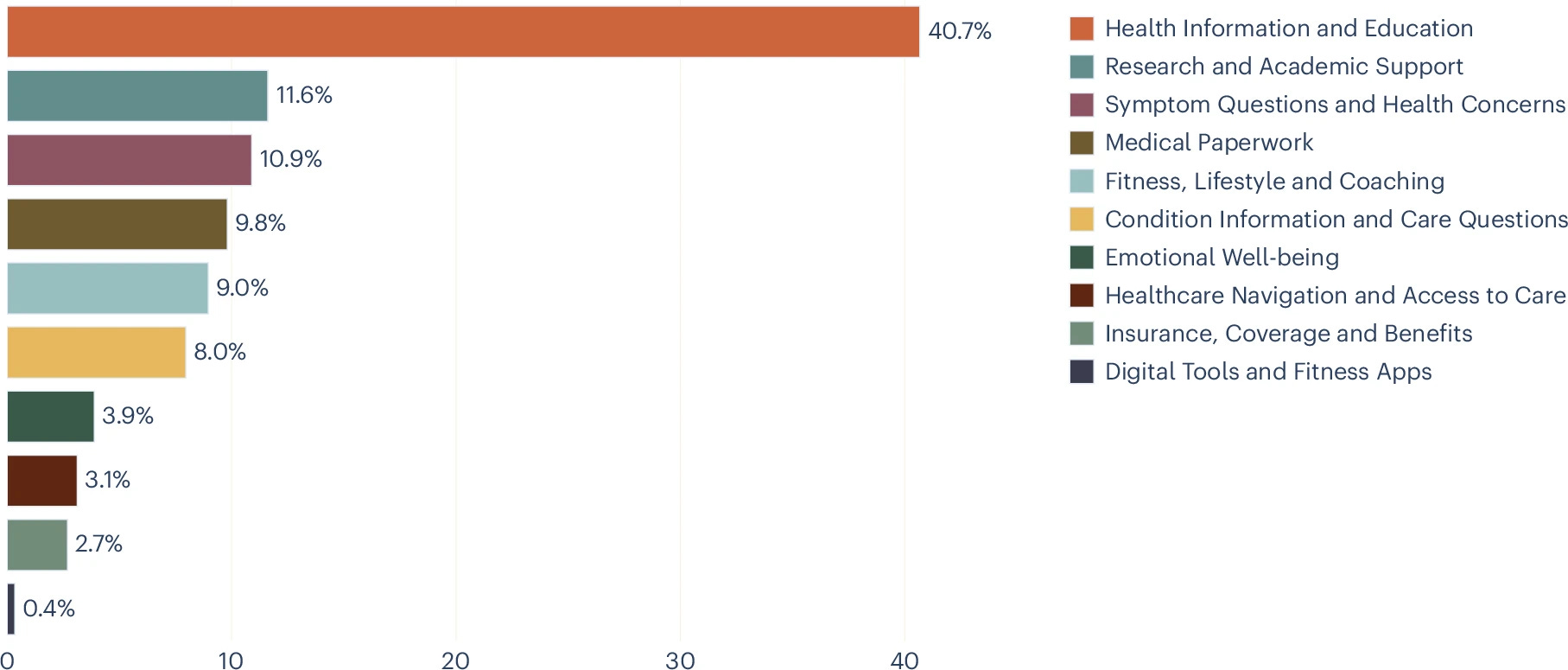
Analysis of 500,000+ Microsoft Copilot health conversations (January 2026): nearly 1 in 5 involve personal symptoms or conditions, and 1 in 7 of those are about someone else. Personal queries spike at night when care is least accessible. Mobile skews personal, desktop skews professional. A large share focus on navigating the system itself: insurance, referrals, logistics. Nature
Why it matters for Longevity Docs: Your patients are running symptoms through Copilot at 11pm the night before their appointment. On mobile. Often for a parent or child. Increasingly to navigate insurance we never trained for. Tomorrow's patient arrives pre-informed, pre-anxious, and pre-diagnosed by an LLM. Be ready.
Anemia and Blood Biomarkers of Alzheimer Disease in Dementia Development

In this cohort study of dementia-free older adults, anemia was associated cross-sectionally with higher levels of AD blood biomarkers and longitudinally with increased dementia risk. The highest dementia risk occurred when low hemoglobin and elevated AD biomarkers coexisted, suggesting a potential interplay between anemia and neuropathology in dementia development. JAMA
Why it matters for Longevity Docs: Anemia is one of the most undertreated findings in adult primary care often dismissed as nutritional or age-related. This data reframes it as a potential accelerant of neurodegeneration, especially when layered onto elevated AD biomarkers. For longevity physicians, that's a clinical mandate: don't stop at the CBC. Pair hemoglobin trends with p-tau217 or GFAP in your high-risk patients, and treat anemia as a cognitive risk factor, not just a hematologic one.
Interferon-related inflammaging links epigenetic age acceleration to multimorbidity
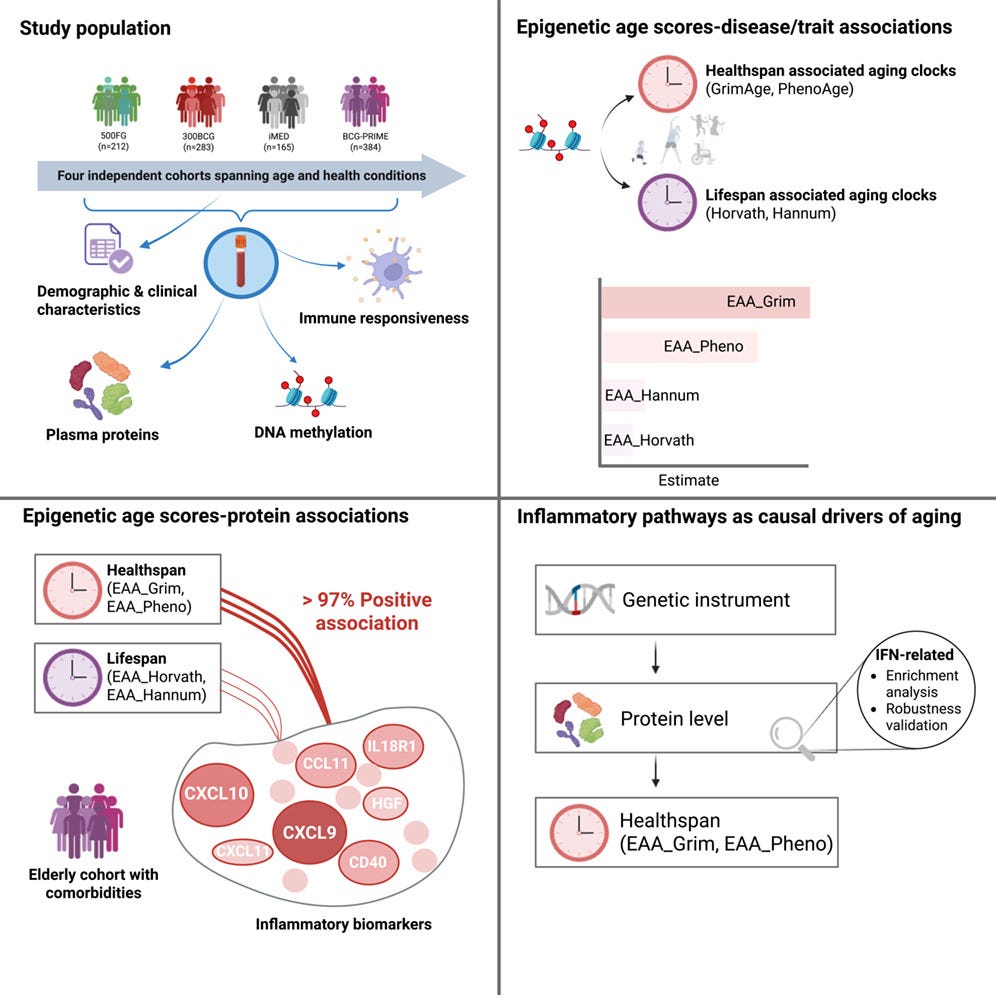
Mendelian randomization shows four interferon-pathway cytokines (CXCL9, CXCL10, CCL11, IL-18) rise with age and causally drive epigenetic age acceleration and age-related disease. Aging also dysregulates immune cytokine production in response to microbial stimulation. The interferon pathway is emerging as a target for anti-aging interventions. Cell
Why it matters for Longevity Docs: Inflammaging has been a useful concept but clinically vague. This paper names four cytokines with a causal Mendelian randomization signal, not just correlation. That moves interferon-pathway inflammation from hypothesis to tractable target. Watch for emerging IFN-modulating interventions and testing.
Electromagnetic field-inducible in vivo gene switch for remote spatiotemporal control of gene expression
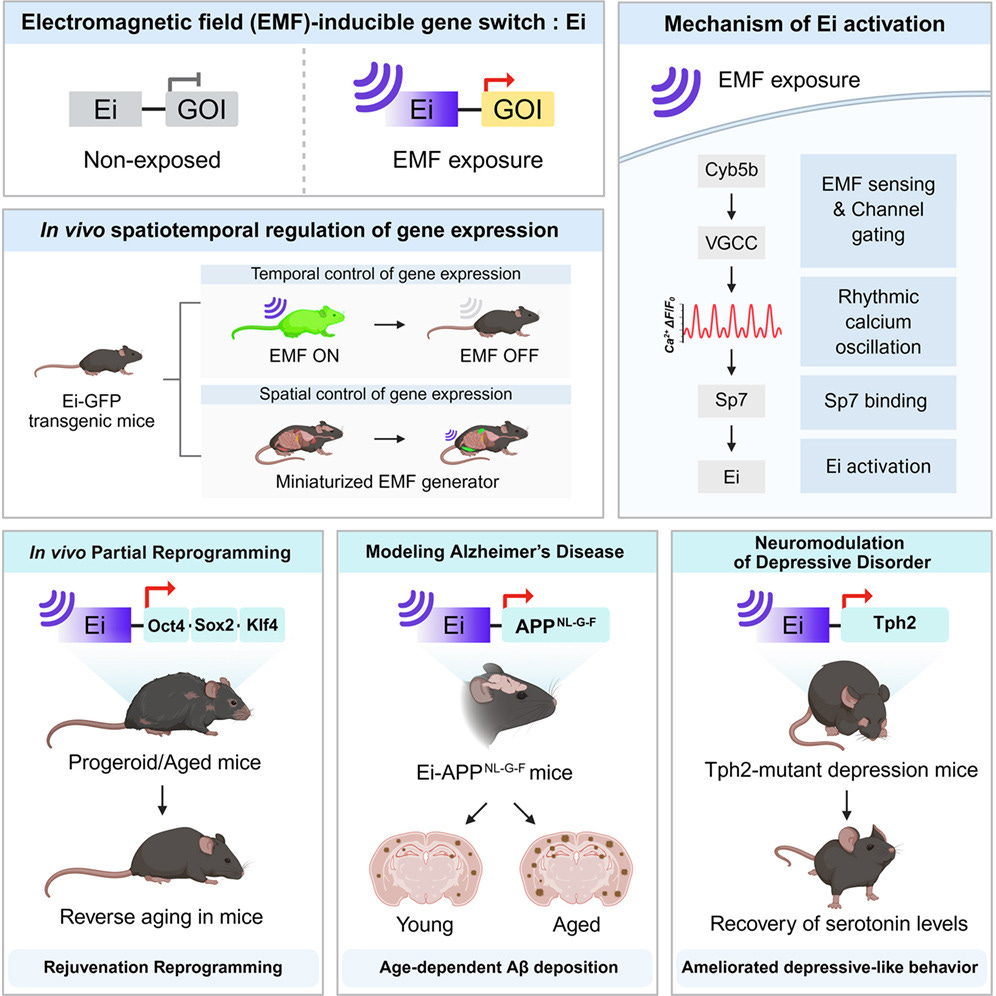
A remotely controlled in vivo gene switch responsive to electromagnetic fields (EMFs) enables precise spatiotemporal gene activation. A CRISPR-Cas9 screen identified cytochrome b5 type B (Cyb5b) as the likely EMF sensor, activated by rhythmic oscillatory calcium dynamics. EMF activation of the Oct4-Sox2-Klf4 (OSK) cassette induced partial reprogramming in aged mice, conditional APP expression recapitulated Alzheimer's pathology, and EMF-mediated Tph2 expression restored serotonergic activity in Tph2-mutant mice. Cell
Why it matters for Longevity Docs: Partial reprogramming via OSK is one of the most discussed frontiers in longevity science, but delivery and control have been the bottleneck. An EMF-triggered, non-invasive switch changes the calculus. You could, in principle, turn on a rejuvenation cassette with external signal precision rather than systemic dosing. Still preclinical, but the delivery architecture is what makes this category eventually clinical. Worth tracking as the bridge between reprogramming biology and deployable therapy.

They Are Certified Longevity Docs (CLD)
Congratulations to the physicians who earned their Certified Longevity Docs (CLD) designation this month. Empowering the next generation of physicians committed to the standard of evidence-based longevity medicine education.
Dr. Sumita Jain — Founder, Corsano Health and Wellness (Zionsville, Indiana)
Ten years in primary care, with a specific commitment to bringing preventive medicine to underserved and underrepresented patients. Proof that longevity medicine belongs in every zip code, not just the wealthy ones.
Dr. Johan Hedevåg — Founder & CEO, Revi Health (Stockholm, Sweden)
One of Scandinavia’s first CLD-certified physicians. Building longevity practice infrastructure in a region where the specialty is still being defined. Founder and CEO of Revi Health, a network of clinics in Sweden, focusing on longevity, regenerative medicine and performance health.
The Certified Longevity Doctor designation is the standard our community is building. If you practice longevity medicine with evidence and accountability, this is the credential that says it.

Every week, I track funding, FDA approvals, product launches, and breakthrough announcements shaping longevity medicine.
CARE
Bryan Johnson Offers Free Biomarkers Testing
Blueprint launched a direct-to-consumer biomarker membership at $365/year: two annual panels, 100+ biomarkers, 160+ measurements. Members get blood draws and urine samples through Quest, a dashboard visualizing results, uploads from past labs, and an AI health companion. Physician review costs extra. Athletechnews
Why it matters for Longevity Docs: Physicians will increasingly compete with platforms, not other physicians. The panel, the dashboard, and the AI companion are being commoditized at $365/year. What stays defensible is the physician who interprets the results, contextualizes them against the patient's life, and builds the plan. Position yourself as the analyst and strategist, not the gatekeeper to labs. Patients will arrive with their Blueprint dashboard open on their phone. Be ready to add the layer they cannot get from a platform.
AI & TECH
Function acquires Getlabs to scale at-home testing

Function Health, the $2.5B membership-based lab testing startup ($365/year, 160+ biomarkers), acquired at-home phlebotomy platform Getlabs on April 10, 2026. Members will soon be able to choose between Quest Diagnostics' 2,200 locations or schedule at-home/in-office draws via Getlabs. Longevity.technology
Why it matters for Longevity Docs: Function is quietly building the consumer rails for preventive medicine — direct-to-patient, subscription-based, geography-agnostic. They've now locked in both the lab network (Quest) and the last-mile collection layer (Getlabs). For longevity physicians, this is the competitive landscape: patients arrive already owning their biomarker data, already enrolled in a consumer brand, already expecting at-home convenience. The physician value is no longer access to testing — it's clinical interpretation, protocol design, and longitudinal care. The question for Longevity Docs is whether CLD physicians plug into this infrastructure or build a physician-led alternative.
POLICIES
FDA moves toward easing restrictions on certain peptides
The FDA will reclassify 12 peptides restricted from compounding since 2023, with advisory panels in July 2026 and February 2027. The first reviews seven peptides including BPC-157. HHS Secretary RFK Jr., a self-described peptide user, framed it as restoring "regulated access." Critics note limited efficacy data and documented adverse events.
Why it matters for Longevity Docs: Patients will walk in asking for BPC-157 by name. Be the physician who can answer with clinical authority, not improvisation. Stay informed, read the news, connect with your community, and deepen your standard of care through our certification.
CULTURE
Climate Action and Healthy Longevity
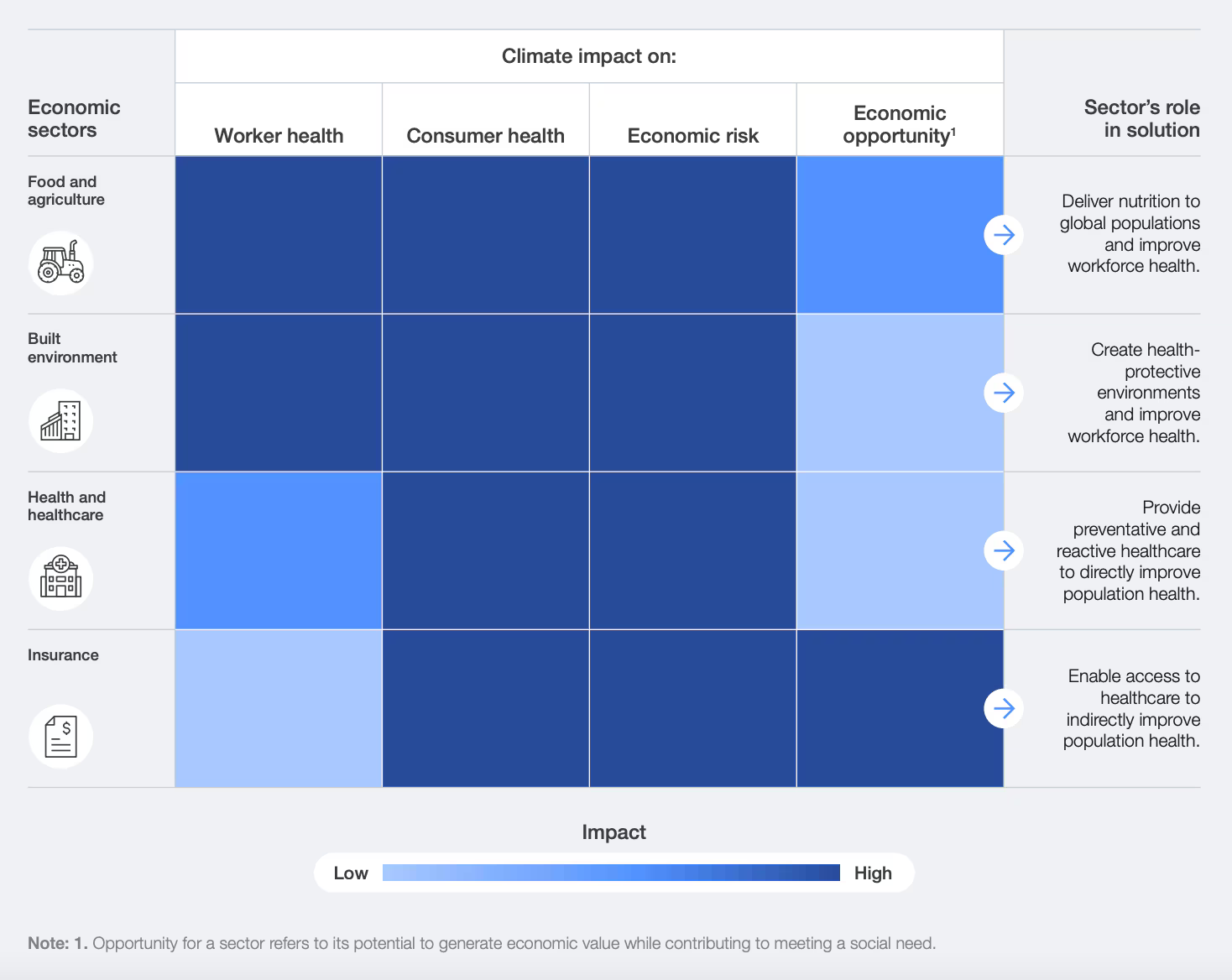
Global life expectancy has more than doubled in a century, but climate change threatens to reverse those gains. The WHO projects ~250,000 additional annual deaths between 2030 and 2050 from heat, undernutrition, malaria, and diarrhea. A widening “longevity gap” is emerging: wealthier, greener neighborhoods outlive hotter, polluted ones by nearly a decade. The call: shift from counting years of life to building climate-resilient years across resilient infrastructure, low-carbon environments, and unified aging + climate policy.
Why it matters for Longevity Docs: Longevity has been built on the individual: labs, biomarkers, protocols. This reframes it as infrastructure. The patient in front of you is also a patient of their zip code, air quality, and heat exposure. Widen the clinical lens and speak into the conversation where longevity meets climate and equity. That is the difference between a specialty and a movement.

Conversations you won’t hear anywhere else.
New Speaker Announcement

Here’s the full speaker block in your order, with learn lines added, cleaned, and ready to paste:
Cannes 2026 Fireside Chats
As promised, the community is growing.
We curated another seven of the most consequential voices in longevity medicine, venture, tech, and healthcare policy. Leaders of industry meet the physicians building the next chapter of longevity medicine. Small group. Physician-focused. Live only.
Dr. Hon Pak, MD, Head of Digital Health, Samsung
The physician shaping how a billion devices become a preventive health platform.
Learn how consumer wearables and AI are redefining the data layer of clinical practice, and what physicians need to own before the platforms do.
Dr. Felix Olale, MD, PhD, Senior Adviser, TPG
Global health investor bridging longevity medicine, equity, and policy on three continents.
Learn how capital is flowing into longevity across continents, and where the physician voice still holds leverage in the global health system.
Elena Bonfiglioli, Healthcare Industry Executive, Microsoft EMEA
The platform layer behind the next decade of health AI, and what it means for physicians.
Learn what the enterprise AI stack looks like inside healthcare, and how physicians can position themselves as the interpretive layer platforms cannot replicate.
Abby Levy, Managing Partner & Co-Founder, Primetime Partners
Venture capitalist shaping the longevity economy. Former senior executive at SoulCycle. Founding President of Thrive Global with Arianna Huffington. Princeton. Harvard Business School.
Learn what venture is funding in longevity, what it is quietly avoiding, and how physicians can build practices that capital respects.
Ali Watson, Partner, LifeSpan MD
Two decades building concierge medicine and longevity before the field had a name. A strategist and operator who has worked with many of the most respected brands in the category. The person founders call when they want to build.
Learn the operational truth of scaling a concierge longevity practice, from one clinic to a network, and the mistakes that cost years.
Dr. Elizabeth Yurth, MD, Co-Founder, Boulder Longevity Institute
One of the most experienced and respected voices in clinical longevity practice. The generation that built the field.
Learn the clinical protocols that have compounded through two decades of practice, and the patterns that still hold after the hype cycles.
Dr. Amanda Kahn, MD
One of New York’s fastest-rising voices in longevity medicine. The generation building what comes next.
Learn how a new physician builds a modern longevity practice from scratch, and what the next decade of clinical longevity actually looks like inside real offices.
Join hundreds of physicians and leaders from Mayo Clinic, Mount Sinai, Samsung, Noom, L’Oréal, ARPA-H, American College of Cardiology
These conversations happen once. In a room you have to be in to hear.
Cannes. June 9–11, 2026. One Room. Limited seats. Curated for physicians
PS: The Back to Medicine visuals drop next week.

Mastermind Replays Now Available

3 Masterminds. 3 topics reshaping longevity practice: AI & Tech, Peptides, and Hormones - featuring the dozens of faculty. Trusted by hundreds of physicians
Conferences
Jun 9–11 — Longevity Docs Cannes: Awards & Summit
Jun 29–Jul 1 — A4LI H-SPAN Summit · Washington, DC Longevity medicine meets regulation and policy.
Aug 24–28 — ARDD · Boston Where aging research meets drug discovery.
Oct 17 — Longevity Docs Skin Longevity Mastermind · New York, NY.

The Home of Longevity Medicine
longevitydocs.™ is the world’s leading longevity physician community - 600+ doctors across 50 countries united by a single conviction: every doctor should be a longevity doctor. Founded by Dr. David Luu, the platform offers its members network, education, and experience with the mission to democratize longevity medicine.
Not a member yet? Join longevitydocs™
We’re a physician-only network. Curated. Vetted. Built on trust. If you’re committed to practicing longevity medicine with rigor, peer support, and shared standards → this is your community. Apply to connect with our team.
Longevity medicine is the personalized, evidence-based practice of modifying the root mechanisms of aging (biological, cognitive, and psychosocial) before they become disease, extending healthspan, not just lifespan. Using advanced diagnostics, precision interventions, and AI-enabled monitoring, it translates measurement into action across every medical discipline. Success is measured in functional capacity, vitality, and disease-free years.

Subscribe to the Longevity Docs Newsletter
Longevity medicine is moving fast. Every week, we bring you what matters: clinical insights, research signals, and perspectives from hundreds physicians across 68+ countries. One newsletter. Built for the physicians shaping this field.
Editorial Disclaimer: