

Acquire Patients Better: The Physician-Patient Fit Checklist
#95 Weekly Longevity Medicine Intelligence

Hey Doc,
Back from Memorial Day weekend. I walked on the beach. Coffee dates with Moana. Met dozens of friends. Amazing dinners, great lunches, crepes for breakfast. I cooked, swam, ran, lifted, did webinars, played games. Friends laughed at me, I made fun of them. Tried golf for the first time with Tayron, talked about the future of the world with family, and laughed a lot too. I lived.
I started writing this newsletter somewhere between the crepes and the pool. Over the weekend I talked to several doctors. The same two problems kept coming up. Some don’t have enough patients to make a good living. Others have too many patients to live a good life. Both feel stuck.
I had a cover story ready on the Enhanced Games and performance medicine. It can wait. The doctors I talked to this weekend aren’t thinking about the Enhanced Games. They’re thinking about Monday morning. So I rewrote this week’s newsletter for them.
How to find the right patients. How to build a practice that sustains you. And how to make sure the life you’re building for your patients is one you’re also living yourself.
Issue 95 is out.
Dr. David Luu, Founder, longevitydocs.™










Each week, I try to explore one idea that could advance longevity medicine and hopefully support physicians in bringing it to life.
Acquire Patients Better: The Physician-Patient Fit Checklist
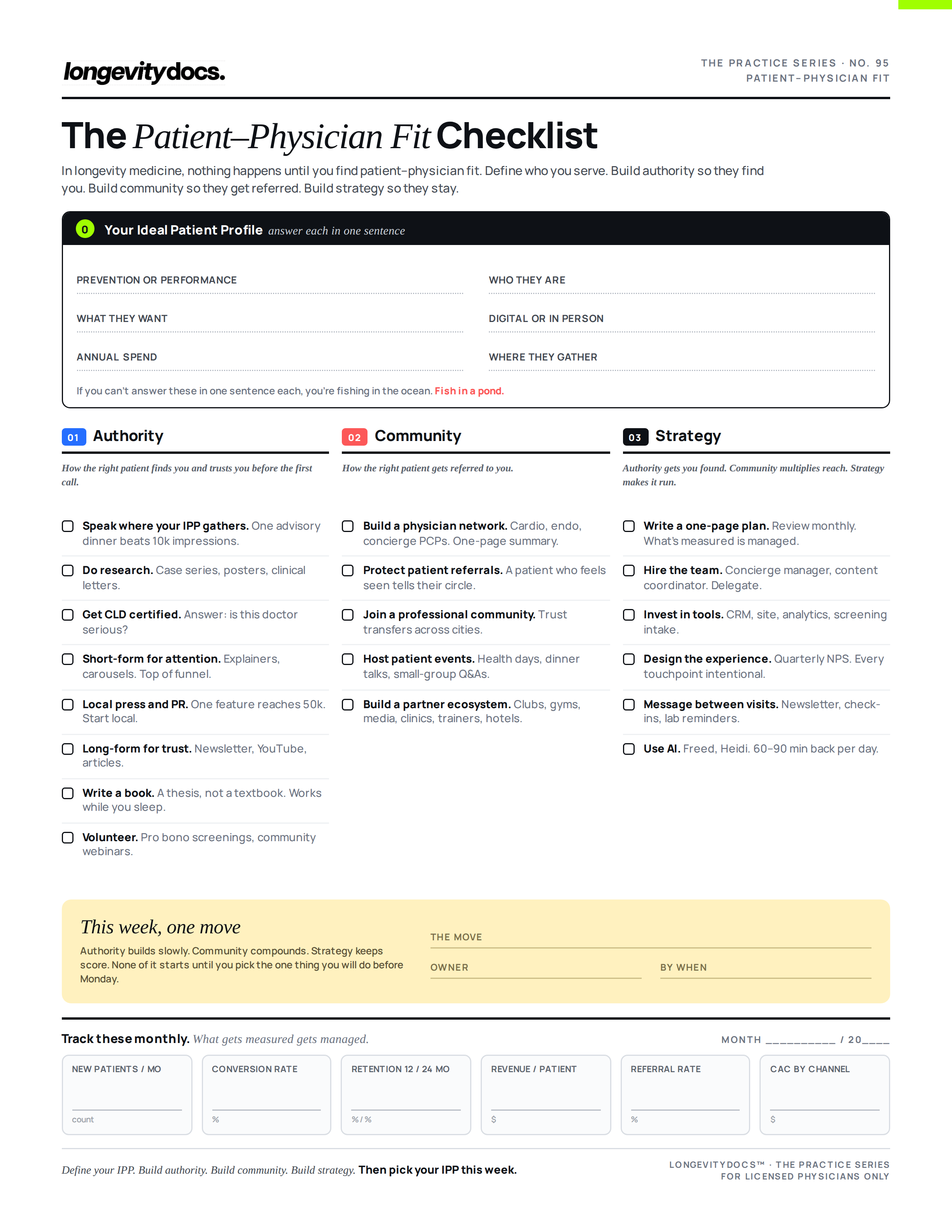
In startups, nothing happens until you find product-market fit. In longevity medicine, nothing happens until you find patient-physician fit (PPF).
Your Ideal Patient Profile (IPP)
Before you build anything, create your IPP by answering questions like these. Prevention or performance? Content creators or hedge fund managers? Weight, hormones, cognition, or annual checkups? Digital or in person? $2K or $20K annually? Social media or country club?
If you can’t answer these in one sentence each, you’re fishing in the ocean. Fish in a pond. Write your IPP on one page. Every decision flows from it.
Pillar 1: Authority
How the right patient finds you and trusts you before the first call.
Speak where your IPP gathers. One talk at a wealth advisory dinner converts better than 10,000 Instagram impressions.
Do research. Case series, posters, clinical letters. Content says you’re informed. Research says you’re contributing.
Become certified. Get your CLD credential. It answers the question every prospective patient is already asking: how do I know this doctor is serious?
Short-form builds attention. 60-second explainers, study carousels, quick commentary. Top of funnel. Earns the click to your long-form.
Local press and PR. One newspaper feature puts you in front of 50,000 people in your market. Start local.
Long-form content builds trust. Monthly newsletter, YouTube, LinkedIn articles. Let the right patient spend 20 minutes inside your clinical thinking before they call.
Write a book. Could be a 50-pages ebook. A clear thesis on how you practice longevity medicine. It works while you sleep.
Volunteer. Free workshops, pro bono screenings, community webinars. Earns trust no marketing budget can buy.
Pillar 2: Community
How the right patient gets referred to you.
Build your physician referral network. Cardiologists, endocrinologists, concierge PCPs. Coffee plus a one-page summary of your practice. Remove every barrier to that referral.
Nuture your patient referral network. A patient who feels seen over years tells their inner circle. That compounds faster than any ad spend.
Join a professional community. Inside Longevitydocs, 1,000+ physicians across 68 countries. A CLD graduate in Miami refers a relocating patient to a CLD graduate in San Francisco. Trust transfers.
Host events. Annual retreat/summit, dinner talks, small-group Q&As. Builds loyalty and generates referrals no platform can replicate.
Build an ecosystem of partners. Country clubs, gyms, media, other clinics, personal trainers, hotels.
Pillar 3: Strategy
Authority gets you found. Community multiplies your reach. Strategy makes it run.
Write a plan. One page. New patients per month, conversion rate, retention at 12 and 24 months, revenue per patient, referral rate, cost per acquisition by channel. Review monthly. What gets measured gets managed.
Hire the team. You cannot be the clinician, marketer, scheduler, and content creator. Hire a concierge manager who owns the patient experience between visits. Contract a content coordinator. Delegate everything that doesn’t require your medical license.
Invest in tools. CRM that tracks every patient touchpoint and referral source. Website that answers three questions (measure, prescribe, relationship). Analytics on every channel. Digital intake forms that screen for fit before you invest time.
Design the experience. NPS survey quarterly. Design every touchpoint: first email after enrollment, lab results delivered with context (not a portal dump), quarterly reviews, annual reassessments. Patients leave practices that feel transactional. They stay in practices that feel intentional.
Message your patients. Monthly newsletter. Quarterly check-in from the concierge manager. Lab reminders before they’re due. Reactivation outreach for patients who lapse. Silence between visits communicates that you only care when they’re paying.
Leverage AI. Documentation tools give you 60 minutes back per day and can compound. AI lab interpretation flags trends across panels. Automated scheduling reduces no-shows. Use AI to expand quality of care, not just volume.
What’s next
Define your IPP. Build authority so that patient finds you. Build community so that patient gets referred to you. Build strategy so that patient stays.
I put it all into a one-page checklist. Adapt it to your practice and your market. Then pick your IPP this week. Everything downstream gets easier once you do.

Every week, the Longevity Docs Chat feels like a front-row seat to the future of medicine. Here’s what had doctors buzzing:
HRT After Breast Cancer with Dr. Jordan Emont
Dr. Emont (OBGYN, Menopause Society-certified, founder of Meridian Medical) argued that millions of breast cancer survivors are denied hormone therapy based on outdated trial data using synthetic progestins, not the bioidentical hormones used today. The key evidence: the Stockholm trial (10-year follow-up) found no increased recurrence in ER-positive patients on tamoxifen + HRT, while HABITS (stopped early, weaker methodology) did. These trials used older regimens, not transdermal estradiol or micronized progesterone.
Key Takeaways:
Breast cancer is not one disease. Receptor status changes the entire risk calculus. ER-negative survivors have front-loaded recurrence in the first 5 years, then less than 1% per year, making HRT conversations very different after that window.
Duavee (conjugated estrogens + bazedoxifene) is underutilized. It acts as a SERM in breast tissue and deserves wider consideration for ER-positive patients who need symptom relief.
Testosterone may be protective. Preclinical data show apoptosis in ER-positive tumors, plus cognitive and mood benefits.
Neurokinin antagonists handle vasomotor and sleep symptoms without systemic hormone exposure in the first 5 years post-diagnosis.
Even low-dose vaginal estradiol (4 mcg Imvexxy) can trigger breast sensitivity in some survivors. Dose matters.
GLP-1 agonists and metformin provide adjunctive anti-growth signaling through insulin sensitization, relevant for survivors with concurrent metabolic risk.
Bottom line: Survivors face greater long-term mortality from cardiovascular disease and osteoporosis than from cancer recurrence, yet are routinely denied HRT. The modern evidence supports individualized risk stratification using receptor status, tumor genetics (ctDNA, Oncotype, Breast Cancer Index), and patient preference over blanket contraindication.
Perimenopausal Weight Loss Resistance with Dr. Catherine Johnson
Dr. Johnson (triple board-certified, obesity medicine + menopause) reframes perimenopause as a precision diagnostic window: the woman gaining weight despite unchanged discipline is showing you her future cardiometabolic, sarcopenic, and osteopenic trajectory in real time. The physiology is estrogen/progesterone chaos producing fragmented sleep, elevated fasting glucose, insulin resistance, and visceral fat accumulation, typically starting in the late 30s and accelerating two years before and after the final period.
Key Takeaways:
BMI lies in perimenopause. Use body composition (body fat ≥30% = overweight regardless of BMI) and HOMA-IR (fasting insulin × fasting glucose ÷ 405) instead.
Screen every perimenopausal woman for Hashimoto’s. It’s present in 20% of this population, and estrogen fluctuation shifts thyroid binding globulins, producing clinical hypothyroidism with normal-looking TSH.
Progesterone first, estrogen last. Progesterone restores sleep and improves insulin sensitivity. Testosterone replacement is deferred until weight is down to avoid fluid retention and growth-factor signaling.
Don’t prescribe exercise first. When cortisol is high, ferritin is low, and sleep is broken, exercise sabotages weight loss in the first six weeks. Fix sleep, nutrients (vitamin D 45-65, ferritin, folate, B12), and cortisol before adding training.
Her SAME framework: Structure (planning), Accountability (data-driven check-ins), Metabolic advantage (insulin sensitizers, GLP-1 agonists, phentermine/topiramate, Vyvanse for binge-eating/brain fog), Environment (social and relational context redesign).
Pharmacologic toolkit spans progesterone, metformin, GLP-1 agonists (500-900 fewer daily calories), Contrave, and phentermine/topiramate ER. She teaches nutritional ketosis with finger-stick ketone monitoring to demonstrate the glycogen-to-fat-oxidation switch.
Quarterly labs to show patients their own fluctuation pattern. Full panel includes androgens, DHEA-S, FSH, estradiol, progesterone, cortisol, insulin, ApoB, Lp(a), full thyroid with binding globulins, celiac screening, and uric acid.
Bottom line: Perimenopause is a systems-level metabolic crisis, not a discipline failure. 40% of a woman’s life is lived postmenopausally, and her trajectory is being written now. Validate her experience, protect her sleep and energy, optimize nutrients and hormones, then build strength. She’ll refer your entire network.

One-Shot Gene Edit Cuts LDL Cholesterol 62% Durably

Verve Therapeutics (now Eli Lilly) published Phase 1 results for VERVE-102, a base-editing therapy that permanently inactivates the PCSK9 gene in the liver via a single IV infusion. At the highest dose, PCSK9 dropped 88% and LDL fell 62% (78 mg/dL), with reductions holding for at least a year. No dose-limiting toxicities. 35 patients with familial hypercholesterolemia or premature CAD.
This is a potential one-and-done replacement for lifelong PCSK9 inhibitor injections. If it holds in larger trials, it fundamentally changes how we manage high-risk lipid patients. NEJM
Retatrutide Hits 30.3% Weight Loss at 104 Weeks
The AJMC piece adds a longer-term data point: patients on 12mg retatrutide lost an average of 85 lbs (30.3%) by week 104, up from the 28.3% at week 80. Even the low 4mg dose delivered 19% loss. The weight loss curve is still trending down past 80 weeks, which matters. It suggests the drug hasn’t plateaued where tirzepatide typically does.
Sleep as a global health priority
Researchers propose treating sleep the way we treat climate or infectious disease: as a planetary health issue requiring coordinated international action. The framework connects human sleep, animal sleep, and environmental exposures (light/noise pollution, climate change, screen time, shift work) into a single model. Key data points: sleep disorders affect roughly a third of the global population, costing $680B annually across five countries, and rising temperatures could strip 50-58 hours of sleep per person per year by century's end. Sleep regularity is a stronger mortality predictor than sleep duration. Cell
AI Predicts Alzheimer’s Trajectory From a Single MRI

Every week, I track funding, FDA approvals, product launches, and breakthrough announcements shaping longevity medicine.
CARE
HSBC Launches Longevity Care

HSBC Singapore is bundling longevity services (health concierge, preventive screenings…) into its premium banking tier through partnerships with IHH Healthcare and Raffles Medical Group.
For longevitydocs: Banks are becoming a distribution channel for longevity medicine. If HSBC is packaging healthspan programs for affluent clients, that’s a new referral pipeline and revenue stream for longevity-trained doctors who can plug into these ecosystems as providers or advisors.
INVESTMENT
Oura Files for IPO

Nourish Raises $100m for AI-native Metabolic Clinic

Nourish, the largest virtual dietitian-led clinic in the US, raised a $100M Series C to expand into physician-led metabolic care, including GLP-1 prescribing and lab testing. The company hit profitability in 2025 and is scaling its physician workforce through 2026.
For longevitydocs: Nutrition-first platforms are moving upstream into your lane. If insurers start routing metabolic patients to Nourish instead of specialist visits, the referral map changes fast.
Kin Health Raises $9M for a Patient-Facing AI Visit Notetaker

Free app records doctor visits, returns AI summaries with action items. Founded by GoodRx/HeyDoctor alumni and two physicians. Monetizes via referral commissions, not subscriptions. Plans to integrate EHR data later this year.
For longevity doctors: Patients will start arriving with AI transcripts of prior visits across multiple providers. Useful for continuity, but watch for hallucinated action items.
CULTURE
Enhanced Games Platform

The Enhanced Games launched in Vegas: openly doped athletes competing in swimming, sprinting, and weightlifting, funded by Silicon Valley at a $1.2B valuation. Results were mostly underwhelming, one swimming world record. The real play is a telehealth business selling testosterone and peptides to consumers.
For longevitydocs: This normalizes supervised performance-enhancing drugs (steroids, testosterone, HGH, peptides, stimulants, etc) and builds consumer demand for those substances. More patients will come asking, the question is whether they come to you or to a DTC app.

Discover who is going Back to Medicine
Longevitydocs Cannes Summit & Awards- June 9-11








































The Home of Longevity Medicine
longevitydocs.™ is the world’s leading longevity physician community - 1,000+ physicians across 68 countries united by a single conviction: every doctor should be a longevity doctor. Founded by Dr. David Luu, the platform offers its members network, education, and experience with the mission to democratize longevity medicine.
Not a member yet? Join longevitydocs™
We’re a physician-only network. Curated. Vetted. Built on trust. If you’re committed to practicing longevity medicine with rigor, peer support, and shared standards → this is your community. Apply to connect with our team.
Longevity medicine is the personalized, evidence-based practice of modifying the root mechanisms of aging (biological, cognitive, and psychosocial) before they become disease, extending healthspan, not just lifespan. Using advanced diagnostics, precision interventions, and AI-enabled monitoring, it translates measurement into action across every medical discipline. Success is measured in functional capacity, vitality, and disease-free years.

Subscribe to the Longevity Docs Newsletter
Longevity medicine is moving fast. Every week, we bring you what matters: clinical insights, research signals, and perspectives from 1,000+ physicians across 68 countries. One newsletter. Built for the physicians shaping this field.
Editorial Disclaimer: